School of Optometry, University of California, Berkeley, CA, USA.
School of Behavioral and Brain Sciences, University of Texas at Dallas, Richardson, TX, USA.
BMC Neurol. 2022 Jul 22;22(1):273. doi: 10.1186/s12883-022-02801-3.
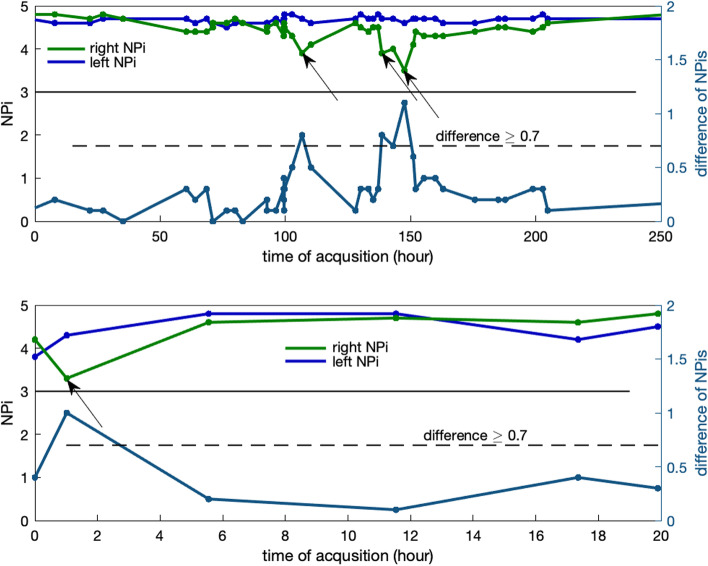
Automated infrared pupillometry (AIP) and the Neurological Pupil index (NPi) provide an objective means of assessing and trending the pupillary light reflex (PLR) across a broad spectrum of neurological diseases. NPi quantifies the PLR and ranges from 0 to 5; in healthy individuals, the NPi of both eyes is expected to be ≥ 3.0 and symmetric. AIP values demonstrate emerging value as a prognostic tool with predictive properties that could allow practitioners to anticipate neurological deterioration and recovery. The presence of an NPi differential (a difference ≥ 0.7 between the left and right eye) is a potential sign of neurological abnormality.
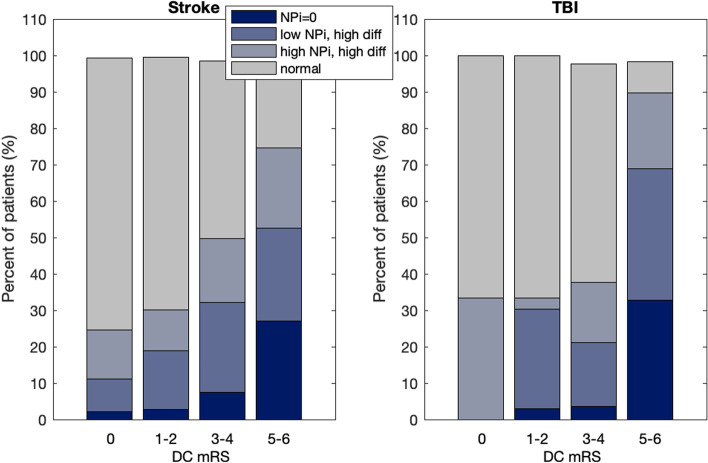
We explored NPi differential by considering the modified Rankin Score at discharge (DC mRS) among patients admitted to neuroscience intensive care units (NSICU) of 4 U.S. and 1 Japanese hospitals and for two cohorts of brain injuries: stroke (including subarachnoid hemorrhage, intracerebral hemorrhage, acute ischemic stroke, and aneurysm, 1,200 total patients) and 185 traumatic brain injury (TBI) patients for a total of more than 54,000 pupillary measurements.
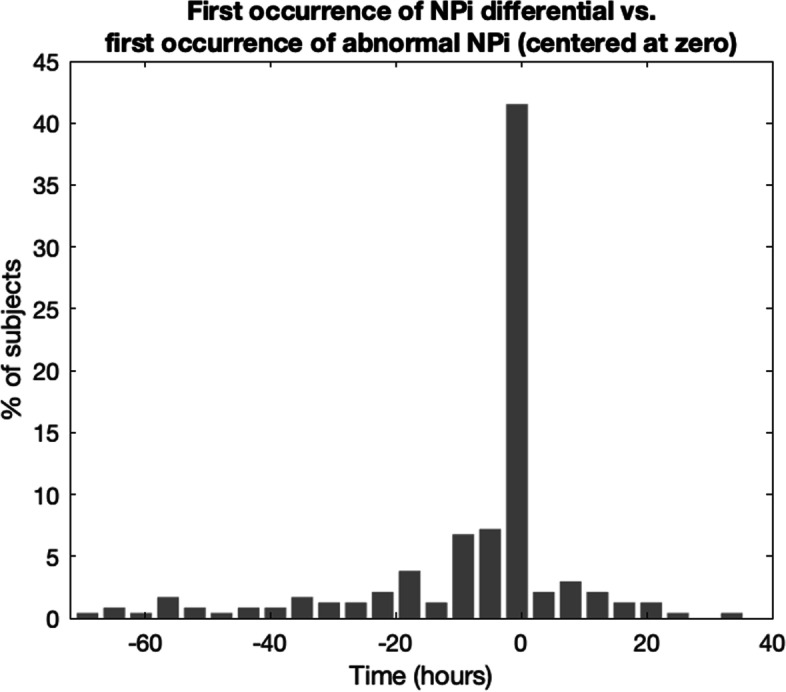
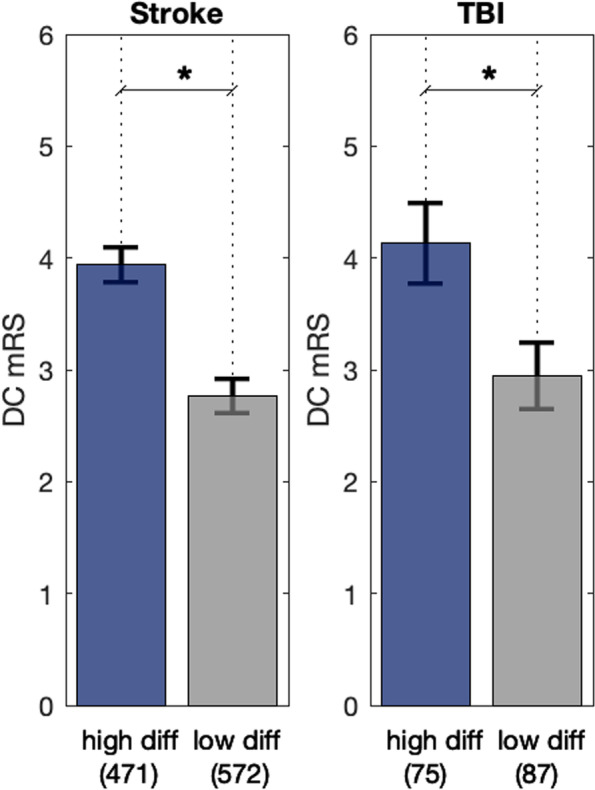
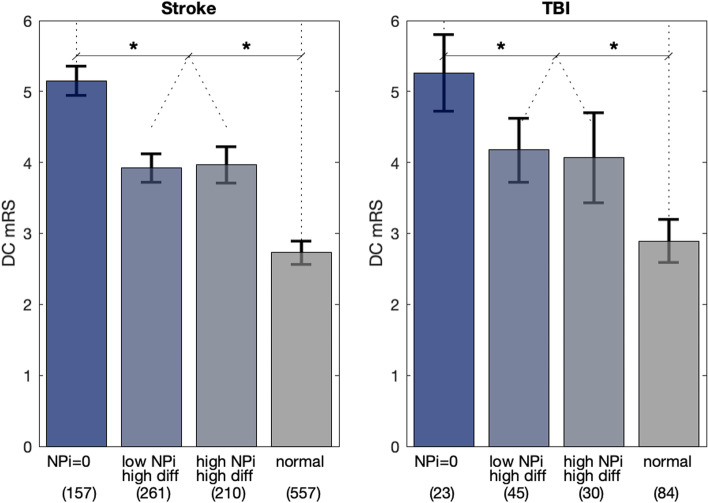
Stroke patients with at least 1 occurrence of an NPi differential during their NSICU stay have higher DC mRS scores (3.9) compared to those without an NPi differential (2.7; P < .001). Patients with TBI and at least 1 occurrence of an NPi differential during their NSICU stay have higher discharge modified Rankin Scale scores (4.1) compared to those without an NPi differential (2.9; P < .001). When patients experience both abnormalities, abnormal (NPi < 3.0) and an NPi differential, the latter has an anticipatory relationship with respect to the former (P < .001 for z-score skewness analysis). Finally, our analysis confirmed ≥ 0.7 as the optimal cutoff value for the NPi differential (AUC = 0.71, P < .001).
The NPi differential is an important factor that clinicians should consider when managing critically ill neurological injured patients admitted to the neurocritical care units.
NCT02804438 , Date of Registration: June 17, 2016.
自动红外瞳孔测量(AIP)和神经瞳孔指数(NPi)为评估和跟踪光反射(PLR)提供了一种客观的方法,涵盖了广泛的神经疾病谱。NPi 量化了 PLR,范围从 0 到 5;在健康个体中,双眼的 NPi 预计为≥3.0 和对称。AIP 值作为一种预后工具具有预测特性,表明它可能允许从业者预测神经恶化和恢复。NPi 差异(左眼和右眼之间的差异≥0.7)的存在是神经异常的潜在迹象。
我们通过考虑美国 4 家医院和日本 1 家医院神经重症监护病房(NSICU)入院患者的改良 Rankin 评分出院时(DC mRS),以及两个脑损伤队列来探索 NPi 差异:中风(包括蛛网膜下腔出血、脑出血、急性缺血性中风和动脉瘤,共 1200 例患者)和 185 例创伤性脑损伤(TBI)患者,共超过 54000 次瞳孔测量。
在 NSICU 期间至少发生 1 次 NPi 差异的中风患者的 DC mRS 评分(3.9)高于未发生 NPi 差异的患者(2.7;P<0.001)。在 NSICU 期间至少发生 1 次 NPi 差异的 TBI 患者的出院改良 Rankin 评分(4.1)高于未发生 NPi 差异的患者(2.9;P<0.001)。当患者同时出现两种异常时,异常(NPi<3.0)和 NPi 差异,后者与前者具有预测关系(z 得分偏度分析的 P<0.001)。最后,我们的分析证实,≥0.7 是 NPi 差异的最佳截断值(AUC=0.71,P<0.001)。
NPi 差异是神经危重症患者管理中临床医生应考虑的一个重要因素。
NCT02804438,登记日期:2016 年 6 月 17 日。