Schuemie Martijn J, Arshad Faaizah, Pratt Nicole, Nyberg Fredrik, Alshammari Thamir M, Hripcsak George, Ryan Patrick, Prieto-Alhambra Daniel, Lai Lana Y H, Li Xintong, Fortin Stephen, Minty Evan, Suchard Marc A
Observational Health Data Sciences and Informatics, New York, NY, United States.
Observational Health Data Analytics, Janssen R&D, Titusville, NJ, United States.
Front Pharmacol. 2022 Jul 6;13:893484. doi: 10.3389/fphar.2022.893484. eCollection 2022.
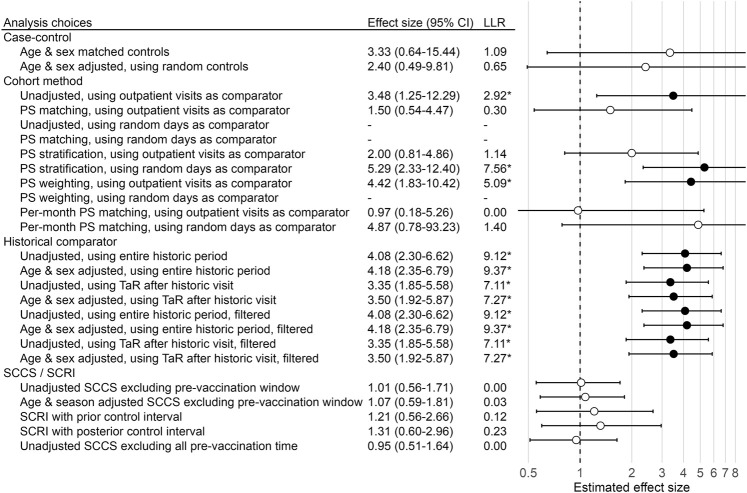
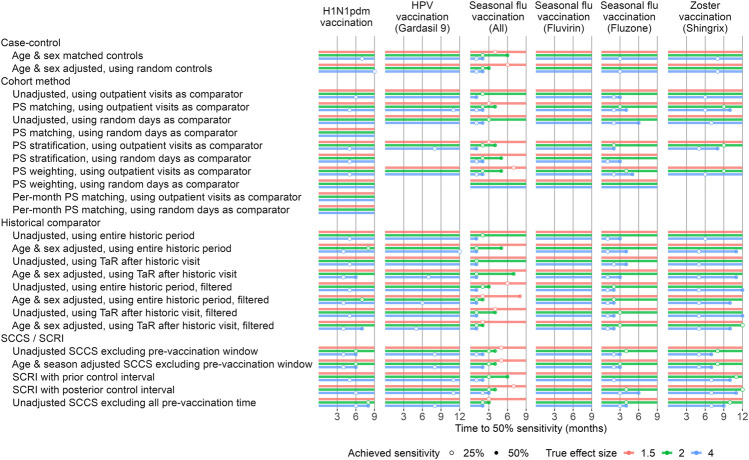
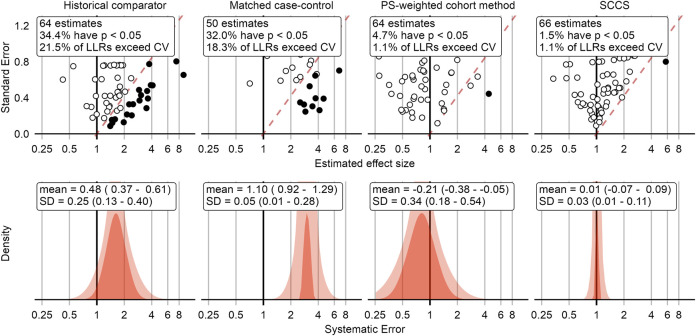
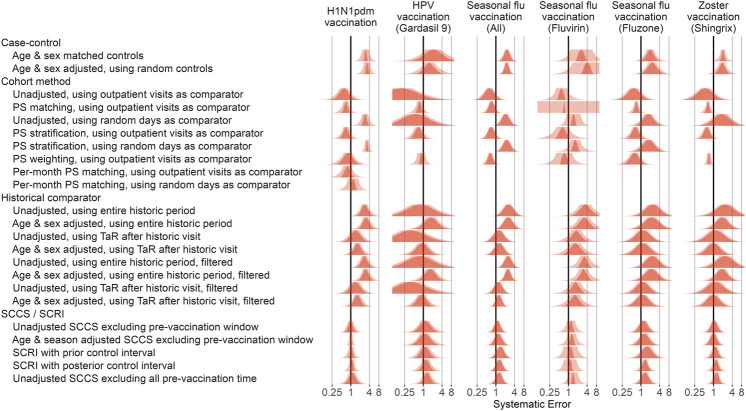
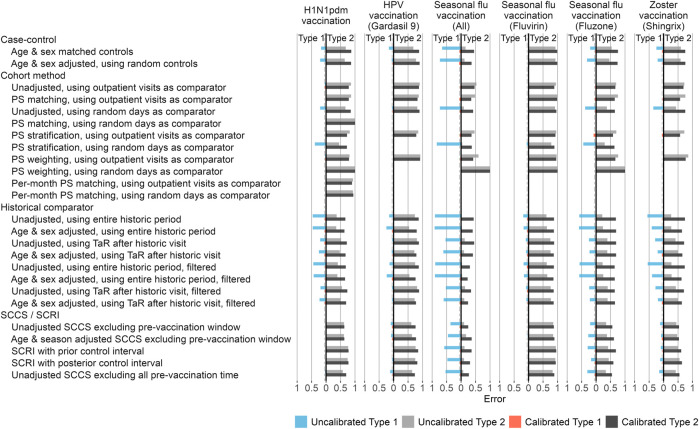
Routinely collected healthcare data such as administrative claims and electronic health records (EHR) can complement clinical trials and spontaneous reports to detect previously unknown risks of vaccines, but uncertainty remains about the behavior of alternative epidemiologic designs to detect and declare a true risk early. Using three claims and one EHR database, we evaluate several variants of the case-control, comparative cohort, historical comparator, and self-controlled designs against historical vaccinations using real negative control outcomes (outcomes with no evidence to suggest that they could be caused by the vaccines) and simulated positive control outcomes. Most methods show large type 1 error, often identifying false positive signals. The cohort method appears either positively or negatively biased, depending on the choice of comparator index date. Empirical calibration using effect-size estimates for negative control outcomes can bring type 1 error closer to nominal, often at the cost of increasing type 2 error. After calibration, the self-controlled case series (SCCS) design most rapidly detects small true effect sizes, while the historical comparator performs well for strong effects. When applying any method for vaccine safety surveillance we recommend considering the potential for systematic error, especially due to confounding, which for many designs appears to be substantial. Adjusting for age and sex alone is likely not sufficient to address differences between vaccinated and unvaccinated, and for the cohort method the choice of index date is important for the comparability of the groups. Analysis of negative control outcomes allows both quantification of the systematic error and, if desired, subsequent empirical calibration to restore type 1 error to its nominal value. In order to detect weaker signals, one may have to accept a higher type 1 error.
常规收集的医疗保健数据,如行政索赔和电子健康记录(EHR),可以补充临床试验和自发报告,以检测疫苗以前未知的风险,但对于早期检测和宣布真正风险的替代流行病学设计的行为仍存在不确定性。使用三个索赔数据库和一个电子健康记录数据库,我们针对历史疫苗接种情况,使用实际阴性对照结果(没有证据表明它们可能由疫苗引起的结果)和模拟阳性对照结果,评估了病例对照、比较队列、历史对照和自我对照设计的几种变体。大多数方法显示出较大的I类错误,经常识别出假阳性信号。队列方法根据比较者索引日期的选择呈现正向或负向偏差。使用阴性对照结果的效应大小估计进行经验校准可以使I类错误更接近名义值,但通常会以增加II类错误为代价。校准后,自我对照病例系列(SCCS)设计能最快速地检测到小的真实效应大小,而历史对照在强效应方面表现良好。在应用任何疫苗安全监测方法时,我们建议考虑系统误差的可能性,特别是由于混杂因素导致的误差,对于许多设计来说,这种误差似乎很大。仅调整年龄和性别可能不足以解决接种疫苗者和未接种疫苗者之间的差异,对于队列方法,索引日期的选择对于组间的可比性很重要。对阴性对照结果的分析既可以量化系统误差,也可以在需要时进行后续的经验校准,以使I类错误恢复到其名义值。为了检测较弱的信号,可能不得不接受更高的I类错误。