Dhouioui Sabrine, Boujelbene Nadia, Ouzari Hadda-Imene, Tizaoui Kalthoum, Zidi Inès
Laboratory Microorganisms and Active Biomolecules, Sciences Faculty of Tunis, University Tunis El Manar, Tunis, Tunisia.
Department of Pathology, Salah Azaiez Institute, Tunis, Tunisia.
Heliyon. 2022 Jul 19;8(7):e09986. doi: 10.1016/j.heliyon.2022.e09986. eCollection 2022 Jul.
BACKGROUND/OBJECTIVE: Conflicting results on the association between HLA-G and digestive cancers were reported. We conducted a meta-analysis to further investigate the true relationship between HLA-G and digestive cancers (DC).
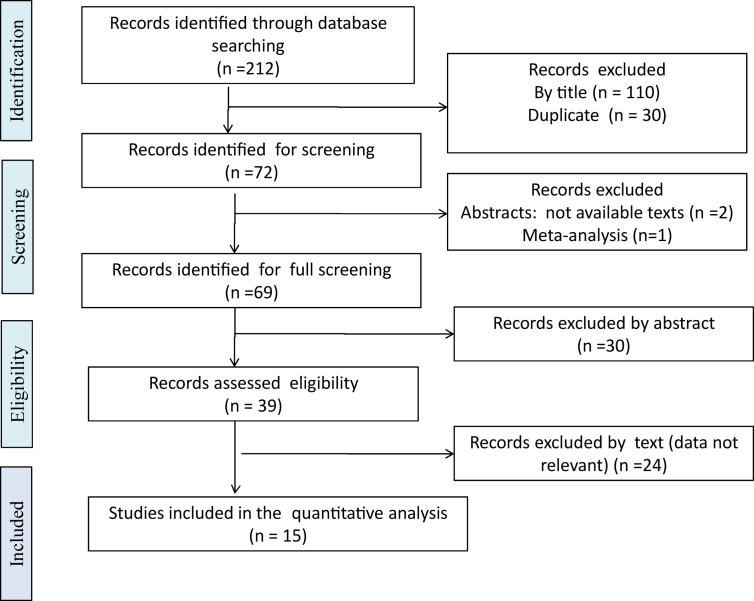
Following PRISMA guidelines, we performed a meta-analysis including 7 case-control studies on HLA-G 14-bp Insertion/deletion (I/D) polymorphism, and 15 studies on soluble HLA-G (sHLA-G). Odds ratios (OR) and their corresponding 95% confidence intervals (CI) for genetic polymorphisms were calculated. The pooled OR was calculated under three genetic models: allelic, recessive, and dominant models. Concerning sHLA-G meta-analysis, standardized mean differences (SMDs) were calculated.
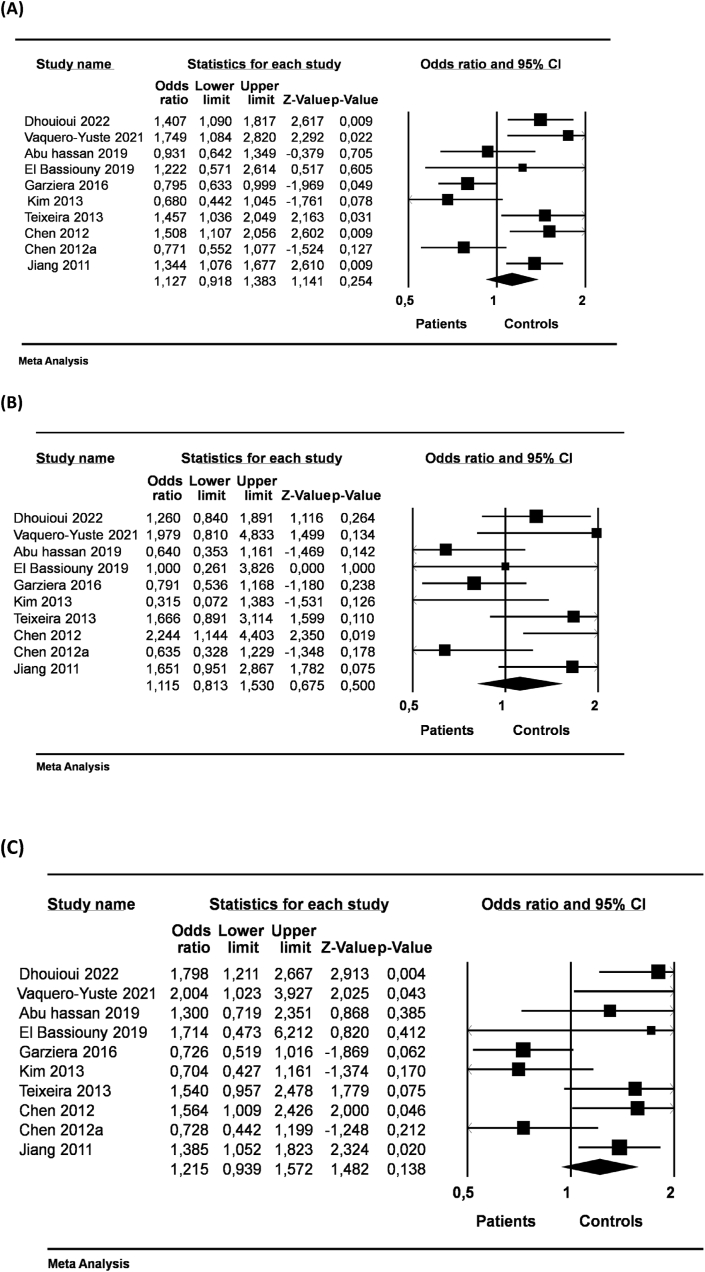
The HLA-G 14-bp I/D was not associated with the risk of DC. However, in the subset of HBV/HCV positive hepato-cellular cancer (HCC) patients, we reported a significant association of HLA-G 14-bp I/D with the disease initiation under allelic (D vs. I; OR = 1.698, 95% CI = 1.263-2.282, p = 0.000), dominant (DD + ID vs. II; OR = 2.321, 95% CI = 1.277-4.218, p = 0.006)and recessive (DD vs. DI + II; OR = 1.739, 95% CI = 1.173-2.577, p = 0.006) genetic models. Interestingly, HLA-G 14-bp I/D was not associated with the disease initiation in HBV/HCV negative HCC patients. However, the infection by HBV/HCV seems to be implicated in the HCC development when we compared HBV/HCV positive patients to HBV/HCV negative patients under allelic (D I; OR = 1.429, 95% CI = 1.029-1.983, p = 0.033, and dominant (DD + ID II; OR = 1.981, 95% CI = 1.002-3.916, p = 0.049) genetic models.Overall analysis of DC showed significant increased sHLA-G in patients compared to healthy controls (SMD = 3.341, 95% CI = 2.415-4.267, p = 0.000). In Asian patients with gastric cancer, sHLA-G was significantly increased in grade 3 compared to low grades (SMD = 0.448, 95% CI = 0.109-0.787, p = 0.000). Further analysis showed that sHLA-G was significantly increased in positive DC vascular invasion (SMD = 0.743, 95% CI = 0.385-1.100, p = 0.000). Accordingly, sHLA-G was associated with a poor prognosis for DC.
The current meta-analysis supports the significant role of HLA-G in DC. The HLA-G 14-bp I/D polymorphism was associated with HCC patients with concomitant HBV/HCV viral infections. Increased sHLA-G indicated a poor prognosis for DC cancer patients.
背景/目的:关于HLA - G与消化系统癌症之间关联的研究结果存在矛盾。我们进行了一项荟萃分析,以进一步探究HLA - G与消化系统癌症(DC)之间的真实关系。
按照PRISMA指南,我们进行了一项荟萃分析,纳入了7项关于HLA - G 14碱基对插入/缺失(I/D)多态性的病例对照研究,以及15项关于可溶性HLA - G(sHLA - G)的研究。计算了基因多态性的优势比(OR)及其相应的95%置信区间(CI)。在三种遗传模型下计算合并OR:等位基因模型、隐性模型和显性模型。对于sHLA - G荟萃分析,计算标准化均数差(SMD)。
HLA - G 14碱基对I/D与DC风险无关。然而,在HBV/HCV阳性肝细胞癌(HCC)患者亚组中,我们报告HLA - G 14碱基对I/D与疾病发生在等位基因模型(D vs. I;OR = 1.698,95% CI = 1.263 - 2.282,p = 0.000)、显性模型(DD + ID vs. II;OR = 2.321,95% CI = 1.277 - 4.218,p = 0.006)和隐性模型(DD vs. DI + II;OR = 1.739,95% CI = 1.173 - 2.577,p = 0.006)下存在显著关联。有趣的是,HLA - G 14碱基对I/D在HBV/HCV阴性HCC患者中与疾病发生无关。然而,当我们在等位基因模型(D vs. I;OR = 1.429,95% CI = 1.029 - 1.983,p = 0.033)和显性模型(DD + ID vs. II;OR = 1.981,95% CI = 1.002 - 3.916,p = 0.049)下比较HBV/HCV阳性患者与HBV/HCV阴性患者时,HBV/HCV感染似乎与HCC发展有关。DC的总体分析显示,与健康对照相比,患者的sHLA - G显著升高(SMD = 3.341,95% CI = 2.415 - 4.267,p = 0.000)。在亚洲胃癌患者中,3级患者的sHLA - G相比于低级别患者显著升高(SMD = 0.448,95% CI = 0.109 - 0.787,p = 0.000)。进一步分析显示,DC血管侵犯阳性时sHLA - G显著升高(SMD = 0.743,95% CI = 0.385 - 1.100,p = 0.000)。因此,sHLA - G与DC的不良预后相关。
当前的荟萃分析支持HLA - G在DC中起重要作用。HLA - G 14碱基对I/D多态性与伴有HBV/HCV病毒感染的HCC患者相关。sHLA - G升高表明DC癌症患者预后不良。