Universidad de Granada, Granada, Spain
Cardiology, Hospital Universitario Virgen de las Nieves, Granada, Spain.
Open Heart. 2022 Jul;9(2). doi: 10.1136/openhrt-2022-002011.
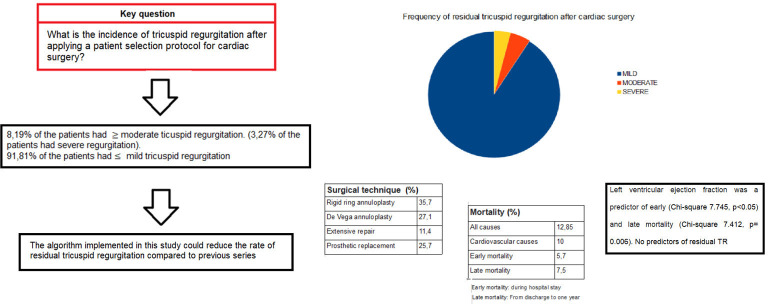
Recurrent tricuspid regurgitation (TR) is frequently observed after cardiac surgery; however, the correct approach remains controversial. We developed an algorithm for action on the tricuspid valve (TV) and conducted a 1-year follow-up study. The aim was to assess the efficacy of the algorithm to minimise residual TR after TV surgery. The hypothesis was that the TR rate at 1 year would be reduced by selecting the surgical approach in accordance with a set of preoperative clinical and echocardiographic variables.
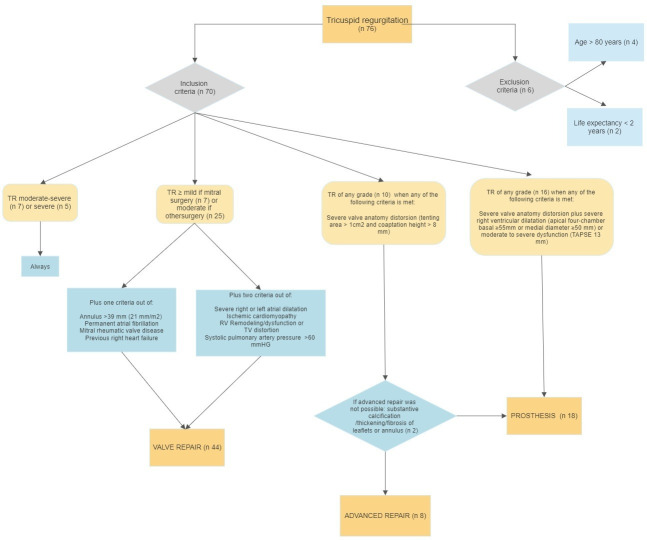
A prospective, observational, single-centre study was performed in 76 consecutive patients with TV involvement. A protocol was designed for their inclusion, and data on their clinical and echocardiographic characteristics were gathered at 3 months and 1-year postsurgery. The treatment of patients depended on the degree of TR. Surgery was performed in all patients with severe or moderate-to-severe TR and in those with mild or moderate TR alongside the presence of certain clinical or echocardiographic factors. They underwent annuloplasty or extended valve repair when the TV was distorted. If repair techniques were not feasible, a prosthesis was implanted. Residual TR rates were compared with published reports, and predictors of early/late mortality and residual TR were evaluated.
TR was functional in 69.9% of patients. Rigid ring annuloplasty was performed in 35.7% of patients, De Vega annuloplasty in 27.1%, extended repair in 11.4% and prosthetic replacement in 25.7%. TR was moderate or worse in 8.19% of patients (severe in 3.27%) at 1 year postintervention. No clinical, surgical or epidemiological variables were significantly associated with residual TR persistence, although annulus diameter showed a close-to-significant association. Total mortality was 12.85% for all causes and 10% for cardiovascular causes. In multivariate analysis, left ventricular ejection fraction was related to both early and late mortality.
Severe residual TR was significantly less frequent than reported in other series, being observed in less than 4% of patients at 1-year postsurgery.
心脏手术后常发生三尖瓣反流(TR)复发;然而,正确的处理方法仍存在争议。我们制定了三尖瓣(TV)手术的处理方案,并进行了为期 1 年的随访研究。目的是评估该方案在最小化 TV 手术后残余 TR 方面的疗效。假设根据术前临床和超声心动图变量选择手术方法可降低 1 年后 TR 发生率。
对 76 例 TV 受累的连续患者进行前瞻性、观察性、单中心研究。设计了一个方案来纳入这些患者,并在术后 3 个月和 1 年收集他们的临床和超声心动图特征数据。患者的治疗取决于 TR 的程度。所有重度或中重度 TR 患者以及轻度或中重度 TR 合并某些临床或超声心动图因素的患者均行手术治疗。TV 变形时行瓣环成形术或扩展瓣叶修复术。如果修复技术不可行,则植入假体。与已发表的报告比较残余 TR 发生率,并评估早期/晚期死亡率和残余 TR 的预测因素。
69.9%的患者为功能性 TR。35.7%的患者行刚性环瓣环成形术,27.1%行 De Vega 瓣环成形术,11.4%行扩展修复术,25.7%行假体置换术。术后 1 年,8.19%(3.27%为重度)的患者 TR 为中重度或更差。尽管瓣环直径接近显著相关,但没有临床、手术或流行病学变量与残余 TR 持续存在显著相关。所有原因的总死亡率为 12.85%,心血管原因的死亡率为 10%。多变量分析显示,左心室射血分数与早期和晚期死亡率均相关。
严重残余 TR 明显少于其他系列报道,术后 1 年时不足 4%的患者存在严重残余 TR。