Departamento de Medicina Intensiva, Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago, Chile.
Escuela de Medicina Veterinaria, Facultad de Ciencias de la Vida, Universidad Andrés Bello, Santiago, Chile.
Sci Rep. 2022 Jul 25;12(1):12648. doi: 10.1038/s41598-022-16446-2.
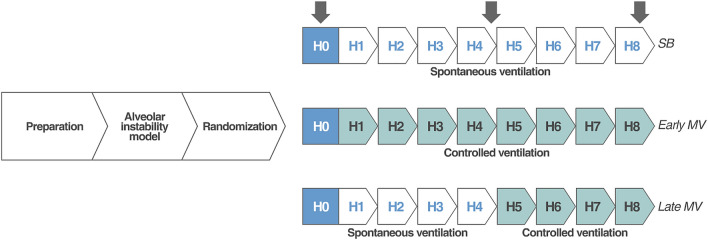
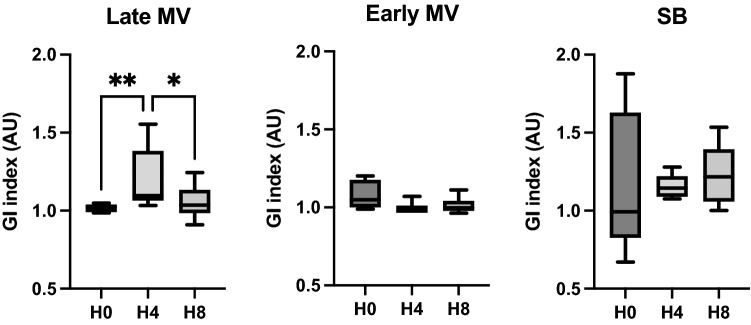
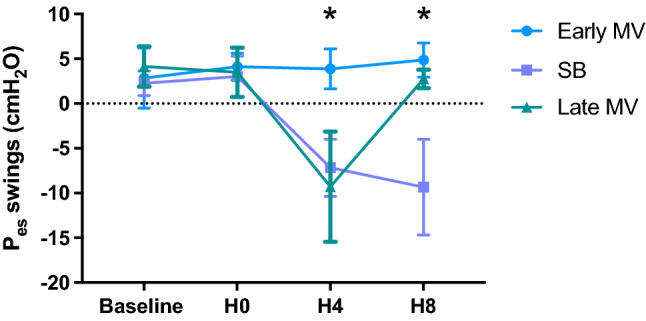
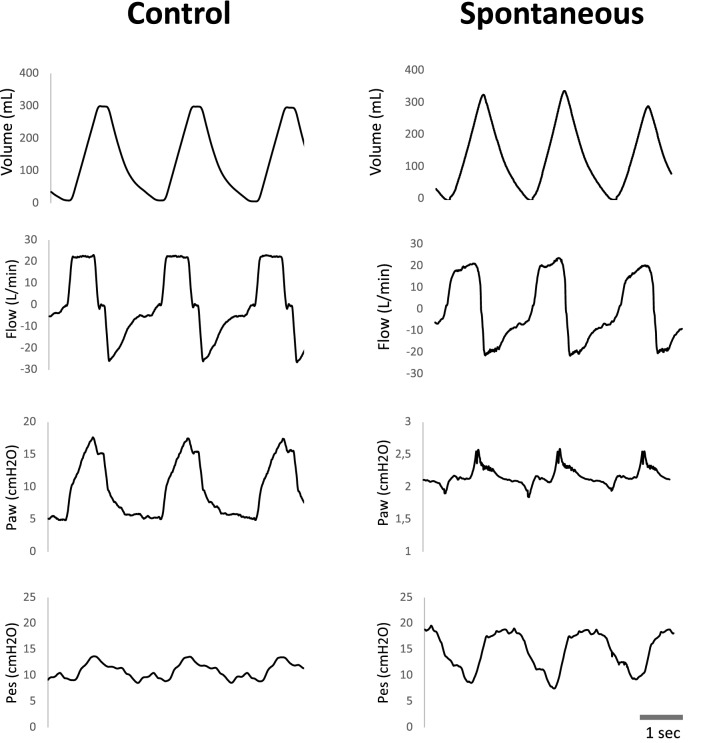
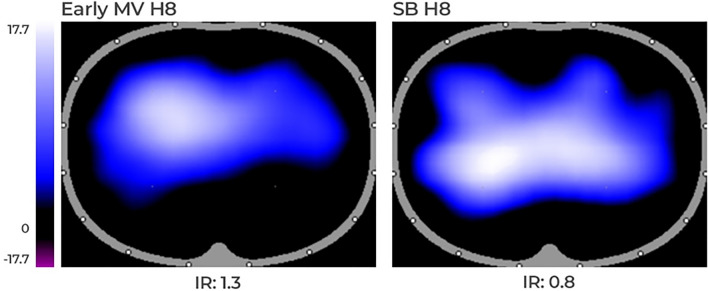
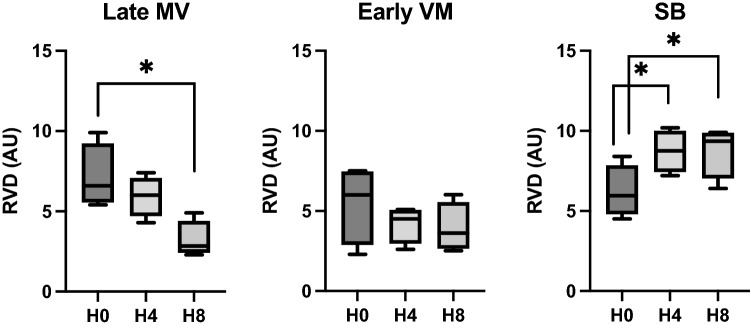
Vigorous spontaneous breathing has emerged as a promotor of lung damage in acute lung injury, an entity known as "patient self-inflicted lung injury". Mechanical ventilation may prevent this second injury by decreasing intrathoracic pressure swings and improving regional air distribution. Therefore, we aimed to determine the effects of spontaneous breathing during the early stage of acute respiratory failure on lung injury and determine whether early and late controlled mechanical ventilation may avoid or revert these harmful effects. A model of partial surfactant depletion and lung collapse was induced in eighteen intubated pigs of 32 ±4 kg. Then, animals were randomized to (1) SB-group: spontaneous breathing with very low levels of pressure support for the whole experiment (eight hours), (2) Early MV-group: controlled mechanical ventilation for eight hours, or (3) Late MV-group: first half of the experiment on spontaneous breathing (four hours) and the second half on controlled mechanical ventilation (four hours). Respiratory, hemodynamic, and electric impedance tomography data were collected. After the protocol, animals were euthanized, and lungs were extracted for histologic tissue analysis and cytokines quantification. SB-group presented larger esophageal pressure swings, progressive hypoxemia, lung injury, and more dorsal and inhomogeneous ventilation compared to the early MV-group. In the late MV-group switch to controlled mechanical ventilation improved the lung inhomogeneity and esophageal pressure swings but failed to prevent hypoxemia and lung injury. In a lung collapse model, spontaneous breathing is associated to large esophageal pressure swings and lung inhomogeneity, resulting in progressive hypoxemia and lung injury. Mechanical ventilation prevents these mechanisms of patient self-inflicted lung injury if applied early, before spontaneous breathing occurs, but not when applied late.
在急性肺损伤中,剧烈的自主呼吸已成为肺损伤的促进因素,这种现象被称为“患者自伤性肺损伤”。机械通气通过降低胸内压力波动和改善区域空气分布,可以防止这种二次损伤。因此,我们旨在确定急性呼吸衰竭早期自主呼吸对肺损伤的影响,并确定早期和晚期控制机械通气是否可以避免或逆转这些有害影响。在 18 头 32 ±4kg 气管插管猪中诱导部分表面活性剂耗竭和肺萎陷模型。然后,动物随机分为(1)SB 组:整个实验(8 小时)均接受极低水平压力支持的自主呼吸;(2)早期 MV 组:接受控制机械通气 8 小时;(3)晚期 MV 组:前半部分实验接受自主呼吸(4 小时),后半部分接受控制机械通气(4 小时)。收集呼吸、血流动力学和电阻抗断层扫描数据。在方案结束后,处死动物,提取肺组织进行组织学分析和细胞因子定量。与早期 MV 组相比,SB 组表现出更大的食管压力波动、进行性低氧血症、肺损伤以及更大的背侧和不均匀通气。在晚期 MV 组切换至控制机械通气可改善肺不均匀性和食管压力波动,但未能预防低氧血症和肺损伤。在肺萎陷模型中,自主呼吸与较大的食管压力波动和肺不均匀性相关,导致进行性低氧血症和肺损伤。如果在自主呼吸发生之前早期应用机械通气,则可以防止这些患者自伤性肺损伤的机制,但如果晚期应用则无法防止。