Cardiology Division, Cardiovascular Department, Ospedale Papa Giovanni XXIII, Bergamo, University of Milan-Bicocca, Milan, Italy.
IdiPaz Research Institute, Hospital La Paz, Universidad Autonoma Madrid, Madrid, Spain.
ESC Heart Fail. 2022 Dec;9(6):3791-3803. doi: 10.1002/ehf2.14050. Epub 2022 Jul 26.
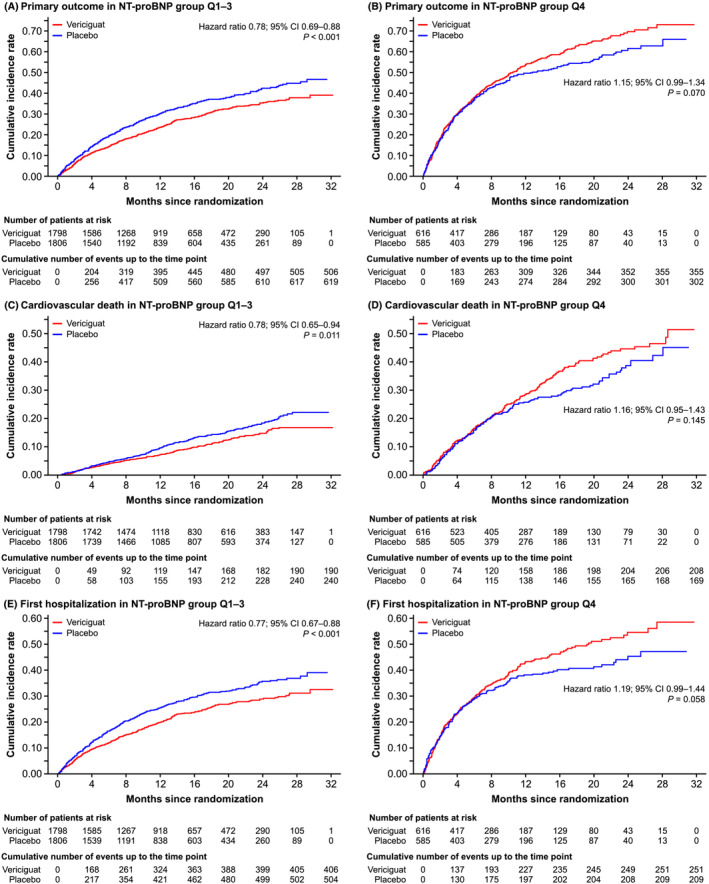
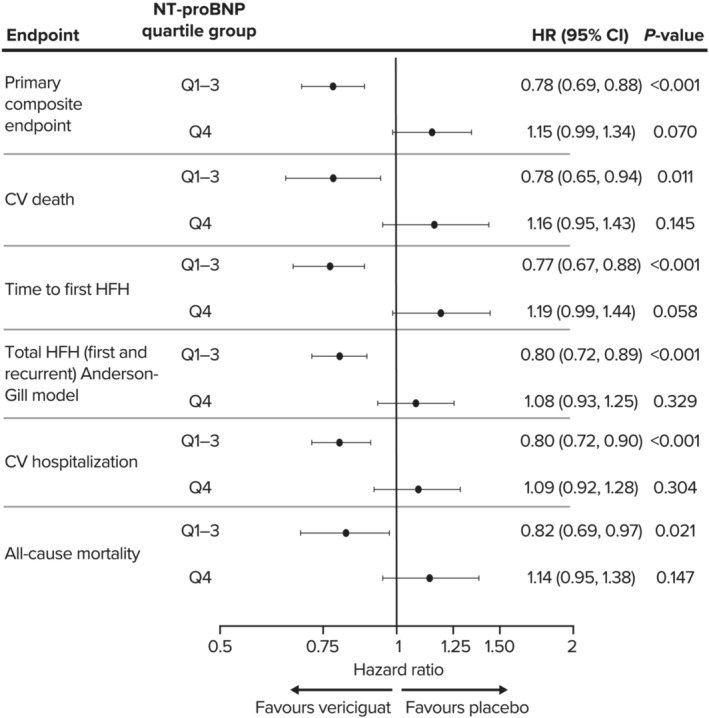
Treatment response to vericiguat, based on baseline N-terminal pro-brain natriuretic peptide (NT-proBNP) subgroups specified in the protocol, was evaluated in the heart failure (HF) VICTORIA trial population by post hoc analysis of combined lower three quartiles [Q1-Q3] vs. the upper quartile [Q4].
VICTORIA participants with available baseline NT-proBNP levels (n = 4805; 95.1% of total) were included. Compared with patients in Q1-Q3 (NT-proBNP: Q1, ≤1556 pg/mL; Q2, >1556-2816 pg/mL; and Q3, >2816-5314 pg/mL), patients in Q4 (NT-proBNP: >5314 pg/mL) were older (69.2 ± 12.0 vs. 66.6 ± 12.1 years), had lower mean ejection fraction (27.2 ± 8.3% vs. 29.5 ± 8.2%; P < 0.0001), and were more likely to be in New York Heart Association (NYHA) Class III (51.8 vs. 35.6%) or IV (2.4 vs. 1.0%). Compared with Q1-Q3, patients in Q4 had higher mean Meta-Analysis Global Group in Chronic Heart Failure risk score (27.3 ± 6.6 vs. 23.5 ± 6.4; P < 0.0001), had lower mean estimated glomerular filtration rate (eGFR; 51.5 ± 25.5 vs. 65.0 ± 26.8 mL/min/1.73 m ; P < 0.0001) and haemoglobin (12.8 ± 2.0 vs. 13.6 ± 1.9 g/dL; P < 0.0001), and more had atrial fibrillation (48.7% vs. 43.1%; P = 0.0007) and were randomized while hospitalized for HF (14.8 vs. 9.9%; P < 0.0001). Target dose was achieved in 72.3 and 63.7% of patients in Q1-Q3 and Q4, respectively (P < 0.0001). Primary outcome (composite of time to cardiovascular death or first HF hospitalization) rates were 24.5 and 31.7 per 100 patient-years for vericiguat and placebo in Q1-Q3 [hazard ratio (HR) 0.78; 95% confidence interval (CI) 0.69-0.88, P < 0.001] and 73.6 and 63.6 in Q4 (HR 1.15; 95% CI 0.99-1.34, P = 0.070). Serious adverse events were more frequent in NT-proBNP Q4 (total population) compared with Q1-Q3 (38.3 vs. 32.3%; P = 0.0001), driven mainly by the placebo group. Adverse events leading to death were more frequent in Q4 than Q1-Q3 (5.8 vs. 2.4%; P < 0.0001).
Plasma NT-proBNP may help identify patients with worsening HF with reduced ejection fraction, in whom the beneficial effects of vericiguat may be highest. Patients with highest NT-proBNP values are probably too far advanced, suffering more co-morbidities, or still clinically unstable after decompensation to derive benefit from vericiguat.
根据方案中规定的基线 N 末端脑利钠肽前体 (NT-proBNP) 亚组,评估心力衰竭 (HF) VICTORIA 试验人群对维立西呱的治疗反应,方法:对有基线 NT-proBNP 水平的 VICTORIA 参与者(n=4805;占总数的 95.1%)进行了事后分析,将联合下三个四分位数(Q1-Q3)与上四分位数(Q4)进行比较。结果:与 Q1-Q3 患者(NT-proBNP:Q1,≤1556pg/mL;Q2,>1556-2816pg/mL;Q3,>2816-5314pg/mL)相比,Q4 患者(NT-proBNP:>5314pg/mL)年龄更大(69.2±12.0 vs. 66.6±12.1 岁),平均射血分数较低(27.2±8.3% vs. 29.5±8.2%;P<0.0001),且更可能处于纽约心脏协会(NYHA)心功能 III 级(51.8% vs. 35.6%)或 IV 级(2.4% vs. 1.0%)。与 Q1-Q3 相比,Q4 患者的平均 Meta-Analysis Global Group in Chronic Heart Failure 风险评分更高(27.3±6.6 vs. 23.5±6.4;P<0.0001),平均估计肾小球滤过率(eGFR;51.5±25.5 vs. 65.0±26.8mL/min/1.73m2;P<0.0001)和血红蛋白(12.8±2.0 vs. 13.6±1.9g/dL;P<0.0001)更低,心房颤动(48.7% vs. 43.1%;P=0.0007)和随机入院心力衰竭(14.8% vs. 9.9%;P<0.0001)的发生率更高。Q1-Q3 和 Q4 组分别有 72.3%和 63.7%的患者达到目标剂量(P<0.0001)。Q1-Q3 组和 Q4 组的主要终点(心血管死亡或首次心力衰竭住院的复合终点)发生率分别为每 100 患者年 24.5%和 31.7%(危险比 [HR] 0.78;95%置信区间 [CI] 0.69-0.88,P<0.001)和 73.6%和 63.6%(HR 1.15;95%CI 0.99-1.34,P=0.070)。与 Q1-Q3 相比,NT-proBNP Q4(总人群)的严重不良事件更为常见(38.3% vs. 32.3%;P=0.0001),主要与安慰剂组有关。与 Q1-Q3 相比,Q4 导致死亡的不良事件更为常见(5.8% vs. 2.4%;P<0.0001)。结论:血浆 NT-proBNP 可能有助于识别射血分数降低的 HF 恶化患者,在这些患者中,维立西呱的有益作用可能最高。NT-proBNP 值最高的患者可能病情进展得更严重,患有更多合并症,或在失代偿后仍处于临床不稳定状态,无法从维立西呱中获益。