From the Departments of Medical Physics (A.D.H., K.J.C., G.P.B., L.A.T., J.K., R.V.C., S.B.F.), Medicine (R.V.C., N.S.), Biostatistics and Medical Informatics (K.E.L.), and Radiology (M.L.S.), University of Wisconsin-Madison, 1111 Highland Ave, Room 1005, Madison, WI 53705; Department of Medicine, University of Texas Southwestern Medical Center, Dallas, Tex (G.P.B.); and Department of Radiology, University of Iowa, Iowa City, Iowa (A.D.H., S.B.F.).
Radiology. 2022 Dec;305(3):688-696. doi: 10.1148/radiol.211433. Epub 2022 Jul 26.
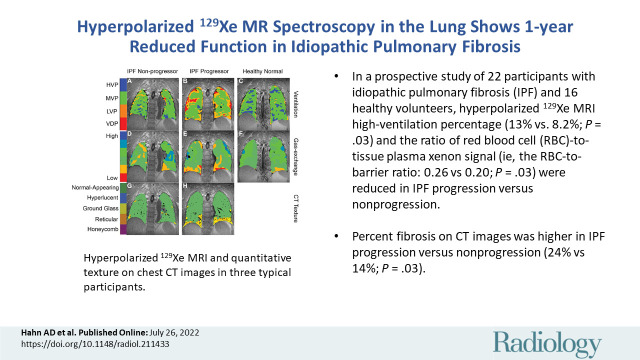
Background Idiopathic pulmonary fibrosis (IPF) is a temporally and spatially heterogeneous lung disease. Identifying whether IPF in a patient is progressive or stable is crucial for treatment regimens. Purpose To assess the role of hyperpolarized (HP) xenon 129 (Xe) MRI measures of ventilation and gas transfer in IPF generally and as an early signature of future IPF progression. Materials and Methods In a prospective study, healthy volunteers and participants with IPF were consecutively recruited between December 2015 and August 2019 and underwent baseline HP Xe MRI and chest CT. Participants with IPF were followed up with forced vital capacity percent predicted (FVC%p), diffusing capacity of the lungs for carbon monoxide percent predicted (DLco%p), and clinical outcome at 1 year. IPF progression was defined as reduction in FVC%p by at least 10%, reduction in DLco%p by at least 15%, or admission to hospice care. CT and MRI were spatially coregistered and a measure of pulmonary gas transfer (red blood cell [RBC]-to-barrier ratio) and high-ventilation percentage of lung volume were compared across groups and across fibrotic versus normal-appearing regions at CT by using Wilcoxon signed rank tests. Results Sixteen healthy volunteers (mean age, 57 years ± 14 [SD]; 10 women) and 22 participants with IPF (mean age, 71 years ± 9; 15 men) were evaluated, as follows: nine IPF progressors (mean age, 72 years ± 7; five women) and 13 nonprogressors (mean age, 70 years ± 10; 11 men). Reduction of high-ventilation percent (13% ± 6.1 vs 8.2% ± 5.9; = .03) and RBC-to-barrier ratio (0.26 ± 0.06 vs 0.20 ± 0.06; = .03) at baseline were associated with progression of IPF. Participants with progressive disease had reduced RBC-to-barrier ratio in structurally normal-appearing lung at CT (0.21 ± 0.07 vs 0.28 ± 0.05; = .01) but not in fibrotic regions of the lung (0.15 ± 0.09 vs 0.14 ± 0.04; = .62) relative to the nonprogressive group. Conclusion In this preliminary study, functional measures of gas transfer and ventilation measured with xenon 129 MRI and the extent of fibrotic structure at CT were associated with idiopathic pulmonary fibrosis disease progression. Differences in gas transfer were found in regions of nonfibrotic lung. © RSNA, 2022 See also the editorial by Gleeson and Fraser in this issue.
背景 特发性肺纤维化(IPF)是一种时空异质性肺部疾病。确定患者的 IPF 是否进展或稳定对于治疗方案至关重要。目的 评估超极化(HP)氙 129(Xe)MRI 通气和气体转移测量在 IPF 中的作用,以及作为未来 IPF 进展的早期特征。材料与方法 在一项前瞻性研究中,2015 年 12 月至 2019 年 8 月连续招募了健康志愿者和 IPF 参与者,并进行了基线 HP Xe MRI 和胸部 CT 检查。对 IPF 参与者进行了 1 年的用力肺活量预测值(FVC%p)、一氧化碳弥散量预测值(DLco%p)和临床结局随访。IPF 进展定义为 FVC%p 至少下降 10%、DLco%p 至少下降 15%或入住临终关怀病房。通过 Wilcoxon 符号秩检验,对 CT 和 MRI 进行空间配准,并比较各组以及 CT 纤维化与正常区域的肺气体转移(红细胞[RBC]-屏障比)和高通气百分比。结果 共评估了 16 名健康志愿者(平均年龄,57 岁±14[SD];10 名女性)和 22 名 IPF 参与者(平均年龄,71 岁±9;15 名男性),其中包括 9 名 IPF 进展者(平均年龄,72 岁±7;5 名女性)和 13 名非进展者(平均年龄,70 岁±10;11 名男性)。基线时高通气百分比(13%±6.1%比 8.2%±5.9%; =.03)和 RBC-屏障比(0.26±0.06 比 0.20±0.06; =.03)的降低与 IPF 的进展有关。进展性疾病患者的 CT 正常结构区域的 RBC-屏障比(0.21±0.07 比 0.28±0.05; =.01)较低,但肺纤维化区域的 RBC-屏障比(0.15±0.09 比 0.14±0.04; =.62)与非进展组无差异。结论 在这项初步研究中,氙 129 MRI 测量的气体转移和通气的功能指标以及 CT 上的纤维化结构程度与特发性肺纤维化的疾病进展相关。在非纤维化肺区发现了气体转移的差异。