Cianciolo Giuseppe, Tondolo Francesco, Barbuto Simona, Angelini Andrea, Ferrara Francesca, Iacovella Francesca, Raimondi Concettina, La Manna Gaetano, Serra Carla, De Molo Chiara, Cavicchi Ottavio, Piccin Ottavio, D'Alessio Pasquale, De Pasquale Loredana, Felisati Giovanni, Ciceri Paola, Galassi Andrea, Cozzolino Mario
Nephrology, Dialysis and Renal Transplant Unit, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Alma Mater Studiorum University of Bologna, Italy.
Interventional, Diagnostic and Therapeutic Ultrasound Unit, Department of Medical and Surgical Sciences, IRCCS Azienda Ospedaliero-Universitaria Sant'Orsola Malpighi Hospital, Bologna, Italy.
Clin Kidney J. 2022 Feb 23;15(8):1459-1474. doi: 10.1093/ckj/sfac050. eCollection 2022 Aug.
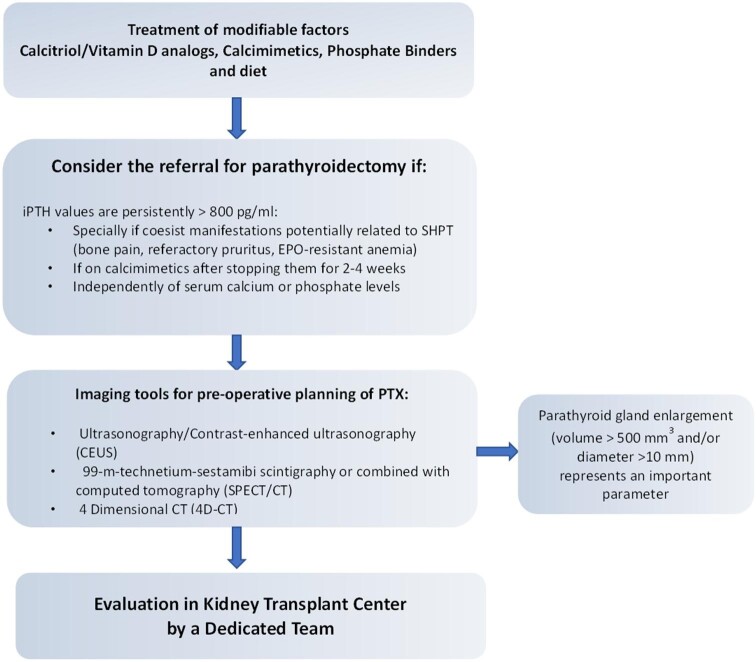
Chronic kidney disease mineral and bone disorder may persist after successful kidney transplantation. Persistent hyperparathyroidism has been identified in up to 80% of patients throughout the first year after kidney transplantation. International guidelines lack strict recommendations about the management of persistent hyperparathyroidism. However, it is associated with adverse graft and patient outcomes, including higher fracture risk and an increased risk of all-cause mortality and allograft loss. Secondary hyperparathyroidism may be treated medically (vitamin D, phosphate binders and calcimimetics) or surgically (parathyroidectomy). Guideline recommendations suggest medical therapy first but do not clarify optimal parathyroid hormone targets or indications and timing of parathyroidectomy. There are no clear guidelines or long-term studies about the impact of hyperparathyroidism therapy. Parathyroidectomy is more effective than medical treatment, although it is associated with increased short-term risks. Ideally parathyroidectomy should be performed before kidney transplantation to prevent persistent hyperparathyroidism and improve graft outcomes. We now propose a roadmap for the management of secondary hyperparathyroidism in patients eligible for kidney transplantation that includes the indications and timing (pre- or post-kidney transplantation) of parathyroidectomy, the evaluation of parathyroid gland size and the integration of parathyroid gland size in the decision-making process by a multidisciplinary team of nephrologists, radiologists and surgeons.
慢性肾脏病矿物质和骨异常在肾移植成功后可能持续存在。在肾移植后的第一年,高达80%的患者被发现存在持续性甲状旁腺功能亢进。国际指南缺乏关于持续性甲状旁腺功能亢进管理的严格建议。然而,它与移植肾及患者的不良结局相关,包括更高的骨折风险以及全因死亡率和移植肾丢失风险增加。继发性甲状旁腺功能亢进可通过药物治疗(维生素D、磷结合剂和拟钙剂)或手术治疗(甲状旁腺切除术)。指南建议首先采用药物治疗,但未阐明甲状旁腺激素的最佳目标值以及甲状旁腺切除术的适应证和时机。关于甲状旁腺功能亢进治疗的影响,尚无明确的指南或长期研究。甲状旁腺切除术比药物治疗更有效,尽管它与短期风险增加相关。理想情况下,甲状旁腺切除术应在肾移植前进行,以预防持续性甲状旁腺功能亢进并改善移植肾结局。我们现提出一份适用于符合肾移植条件患者的继发性甲状旁腺功能亢进管理路线图,其中包括甲状旁腺切除术的适应证和时机(肾移植前或肾移植后)、甲状旁腺大小的评估以及由肾病学家、放射科医生和外科医生组成的多学科团队将甲状旁腺大小纳入决策过程。