Grauer Ralph, Gorin Michael A, Sood Akshay, Butaney Mohit, Olson Phil, Farah Guillaume, Hanna Cole Renee, Jeong Wooju, Abdollah Firas, Menon Mani
Department of Urology, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
Urology, Urology Associates and UPMC Western Maryland, Cumberland, Maryland, USA.
BMJ Surg Interv Health Technol. 2022 Jul 6;4(1):e000122. doi: 10.1136/bmjsit-2021-000122. eCollection 2022.
To assess the impact of iterative changes in preoperative and postoperative biopsy techniques on the outcomes of men undergoing the precision prostatectomy procedure. Precision prostatectomy is a novel surgical treatment for prostate cancer that aims to maximally preserve erectogenic nerves via partial preservation of the prostate capsule.
Retrospective.
Single tertiary care center.
This study included 120 patients who consented to undergo prostate cancer treatment with the precision prostatectomy procedure. Patients were originally enrolled in one of two separate prospective protocols studying precision prostatectomy.
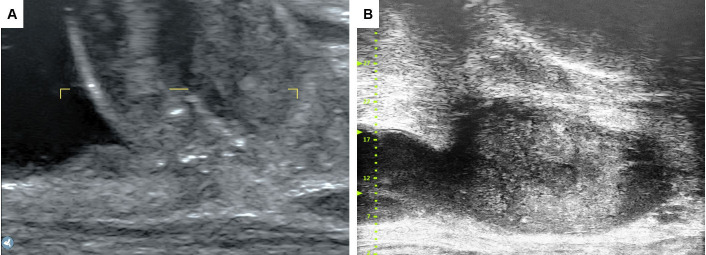
Preoperatively, 60 patients were screened with transrectal (TR) biopsy and 60 were screened by transperineal (TP) biopsy. Ultimately, 117 patients underwent precision prostatectomy. Of the 43 postoperative biopsies, 19 were TR; 17 were TP with ultrasound; and 7 were TP with microultrasound (mUS).
Preoperatively, we evaluated whether the transition to TP biopsy was associated with differences in postoperative treatment failure defined as a neoplasm-positive postoperative biopsy. Postoperative biopsies were compared with respect to their ability to sample the remnant tissue, specifically percentage of cores positive for prostate tissue.
Preoperatively, 9/60 (15%) positive postoperative biopsies occurred in the TR group and 6/60 (10%) in the TP group; Kaplan-Meier survival estimates did not differ between groups (p=0.69 by log rank). Postoperatively, the numbers of cores positive for prostate tissue were 99/160 (62%), 63/107 (59%), and 36/39 (92%) in the TR biopsy, TP with ultrasound, and TP with mUS groups, respectively; this difference was statistically significant versus the rate in the TR and standard TP groups (p=0.0003 and 0.0002).
We found no significant improvement in patient screening, preoperatively-though limited by small sample size and relatively short follow-up. The incorporation of high-frequency mUS for postoperative biopsies improved the ability to sample the remnant tissue with a higher efficiency.
评估术前和术后活检技术的迭代变化对接受精准前列腺切除术男性患者治疗结果的影响。精准前列腺切除术是一种新型的前列腺癌手术治疗方法,旨在通过部分保留前列腺包膜最大限度地保留勃起神经。
回顾性研究。
单一三级医疗中心。
本研究纳入了120例同意接受精准前列腺切除术治疗前列腺癌的患者。患者最初参加了两项单独的研究精准前列腺切除术的前瞻性方案之一。
术前,60例患者接受经直肠(TR)活检筛查,60例接受经会阴(TP)活检筛查。最终,117例患者接受了精准前列腺切除术。在43例术后活检中,19例为TR活检;17例为超声引导下TP活检;7例为微超声(mUS)引导下TP活检。
术前,我们评估了向TP活检的转变是否与定义为术后活检肿瘤阳性的术后治疗失败差异相关。对术后活检在取样残余组织的能力方面进行比较,特别是前列腺组织阳性芯的百分比。
术前,TR组9/60(15%)术后活检阳性,TP组6/60(10%);两组的Kaplan-Meier生存估计无差异(对数秩检验p=0.69)。术后,TR活检组、超声引导下TP活检组和mUS引导下TP活检组前列腺组织阳性芯数量分别为99/160(62%)、63/107(59%)和36/39(92%);与TR活检组和标准TP活检组相比,这一差异具有统计学意义(p=0.0003和0.0002)。
尽管受样本量小和随访时间相对较短的限制,我们发现术前患者筛查无显著改善。在术后活检中采用高频mUS提高了取样残余组织的效率。