Department of Surgery and Transplantation, University Hospital Zurich, Zurich, Switzerland.
Department of General, Abdominal and Transplant Surgery, Croix-Rousse Hospital, Lyon, France.
Ann Surg. 2022 Nov 1;276(5):860-867. doi: 10.1097/SLA.0000000000005634. Epub 2022 Jul 27.
To define benchmark cutoffs for redo liver transplantation (redo-LT).
In the era of organ shortage, redo-LT is frequently discussed in terms of expected poor outcome and wasteful resources. However, there is a lack of benchmark data to reliably evaluate outcomes after redo-LT.
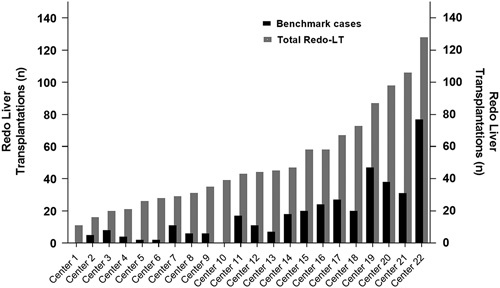
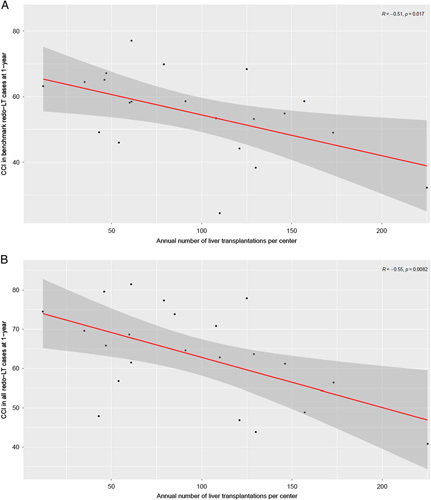
We collected data on redo-LT between January 2010 and December 2018 from 22 high-volume transplant centers. Benchmark cases were defined as recipients with model of end stage liver disease (MELD) score ≤25, absence of portal vein thrombosis, no mechanical ventilation at the time of surgery, receiving a graft from a donor after brain death. Also, high-urgent priority and early redo-LT including those for primary nonfunction (PNF) or hepatic artery thrombosis were excluded. Benchmark cutoffs were derived from the 75th percentile of the medians of all benchmark centers.
Of 1110 redo-LT, 373 (34%) cases qualified as benchmark cases. Among these cases, the rate of postoperative complications until discharge was 76%, and increased up to 87% at 1-year, respectively. One-year overall survival rate was excellent with 90%. Benchmark cutoffs included Comprehensive Complication Index CCI ® at 1-year of ≤72, and in-hospital and 1-year mortality rates of ≤13% and ≤15%, respectively. In contrast, patients who received a redo-LT for PNF showed worse outcomes with some values dramatically outside the redo-LT benchmarks.
This study shows that redo-LT achieves good outcome when looking at benchmark scenarios. However, this figure changes in high-risk redo-LT, as for example in PNF. This analysis objectifies for the first-time results and efforts for redo-LT and can serve as a basis for discussion about the use of scarce resources.
定义再次肝移植(redo-LT)的基准截止值。
在器官短缺的时代,再次肝移植经常被讨论,认为其预后不良且浪费资源。然而,缺乏可靠评估再次肝移植后结果的基准数据。
我们从 22 个高容量移植中心收集了 2010 年 1 月至 2018 年 12 月期间进行的再次肝移植的数据。基准病例定义为终末期肝病模型(MELD)评分≤25、无门静脉血栓形成、手术时无机械通气、接受脑死亡供体的移植物的受者。此外,排除了高紧急优先级和早期再次肝移植,包括原发性无功能(PNF)或肝动脉血栓形成。基准截止值是从所有基准中心中位数的第 75 个百分位数推导出来的。
在 1110 例再次肝移植中,373 例(34%)符合基准病例标准。在这些病例中,术后并发症直至出院的发生率为 76%,分别在 1 年时增加至 87%。1 年总生存率非常高,为 90%。基准截止值包括 1 年时综合并发症指数 CCI ® ≤72,住院和 1 年死亡率分别为≤13%和≤15%。相比之下,接受 PNF 再次肝移植的患者预后较差,某些数值明显超出再次肝移植的基准。
本研究表明,在考虑基准情况时,再次肝移植可获得良好的结果。然而,在高危再次肝移植中,例如 PNF,情况会发生变化。这种分析首次客观地评估了再次肝移植的结果和努力,可以为讨论稀缺资源的使用提供依据。