CIBER of Frailty and Healthy Ageing, CIBERFES, Instituto de Salud Carlos III, Madrid, Spain.
Biomedical Research Foundation, Getafe University Hospital, Carretera de Toledo, Madrid, Spain.
J Cachexia Sarcopenia Muscle. 2022 Oct;13(5):2352-2360. doi: 10.1002/jcsm.13055. Epub 2022 Jul 28.
Frailty and sarcopenia are age-associated syndromes that have been associated with the risk of several adverse events, mainly functional decline and death, that usually coexist. However, the potential role of one of them (sarcopenia) in modulating some of those adverse events associated to the other one (frailty) has not been explored. The aim of this work is to assess the role of sarcopenia within the frailty transitions and mortality in older people.
Data from the Toledo Study of Healthy Aging (TSHA) were used. TSHA is a cohort of community-dwelling older adults ≥65. Frailty was assessed according with the Frailty Phenotype (FP) and the Frailty Trait Scale-5 (FTS5) at baseline and at follow-up. Basal sarcopenia status was measured with the standardized Foundation for the National Institutes of Health criteria. Fisher's exact test and logistic regression model were used to determine if sarcopenia modified the transition of frailty states (median follow-up of 2.99 years) and Cox proportional hazard model was used for assessing mortality.
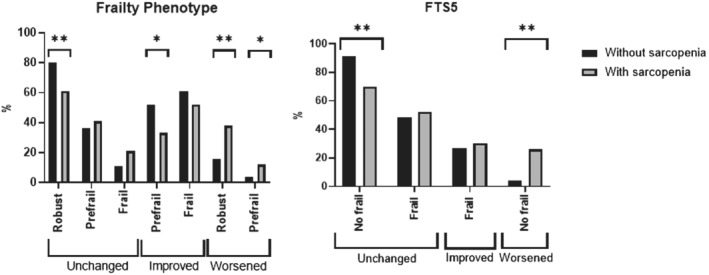
There were 1538 participants (74.73 ± 5.73; 45.51% men) included. Transitions from robustness to prefrailty and frailty according to FP were more frequent in sarcopenic than in non-sarcopenic participants (32.37% vs. 15.18%, P ≤ 0.001; 5.76% vs. 1.12%; P ≤ 0.001, respectively) and from prefrailty-to-frailty (12.68% vs. 4.27%; P = 0.0026). Improvement from prefrail-to-robust and remaining robust was more frequent in non-sarcopenic participants (52.56% vs. 33.80%, P ≤ 0.001; 80.18% vs 61.15%, P ≤ 0.001, respectively). When classified by FTS5, this was also the case for the transition from non-frail-to-frail (25.91% vs. 4.47%, P ≤ 0.001) and for remaining stable as non-frail (91.25% vs. 70.98%, P ≤ 0.001). Sarcopenia was associated with an increased risk of progression from robustness-to-prefrailty [odds ratio (OR) 2.34 (95% confidence interval, CI) (1.51, 3.63); P ≤ 0.001], from prefrailty-to-frailty [OR(95% CI) 2.50 (1.08, 5.79); P = 0.033] (FP), and from non-frail-to-frail [OR(95% CI) 4.73 (2.94, 7.62); P-value ≤ 0.001]. Sarcopenia does not seem to modify the risk of death associated with a poor frailty status (hazard ratios (HR, 95%) P > 0.05).
Transitions within frailty status, but not the risk of death associated to frailty, are modulated by the presence of sarcopenia.
衰弱和肌少症是与多种不良事件相关的年龄相关综合征,主要是功能下降和死亡,通常并存。然而,其中一种(肌少症)在调节与另一种(衰弱)相关的一些不良事件中的潜在作用尚未得到探索。本研究旨在评估肌少症在老年人衰弱转变和死亡中的作用。
使用托莱多健康老龄化研究(TSHA)的数据。TSHA 是一个≥ 65 岁的社区居住老年人队列。根据衰弱表型(FP)和 5 项衰弱特征量表(FTS5)在基线和随访时评估衰弱。基础肌少症状态采用国立卫生研究院标准化标准进行测量。Fisher 确切检验和 logistic 回归模型用于确定肌少症是否改变衰弱状态的转变(中位随访 2.99 年),Cox 比例风险模型用于评估死亡率。
共纳入 1538 名参与者(74.73±5.73;45.51%为男性)。根据 FP,从健壮到虚弱前期和衰弱的转变在肌少症患者中比非肌少症患者更为频繁(32.37%比 15.18%,P≤0.001;5.76%比 1.12%,P≤0.001),从虚弱前期到衰弱(12.68%比 4.27%,P=0.0026)。非肌少症患者从虚弱前期到健壮和保持健壮的改善更为频繁(52.56%比 33.80%,P≤0.001;80.18%比 61.15%,P≤0.001)。当按 FTS5 分类时,非虚弱到虚弱的转变(25.91%比 4.47%,P≤0.001)和保持非虚弱状态稳定(91.25%比 70.98%,P≤0.001)也是如此。肌少症与从健壮到虚弱前期的进展风险增加相关[比值比(OR)2.34(95%置信区间,CI)(1.51,3.63);P≤0.001],从虚弱前期到衰弱[OR(95%CI)2.50(1.08,5.79);P=0.033](FP),从非虚弱到虚弱[OR(95%CI)4.73(2.94,7.62);P 值≤0.001]。肌少症似乎不会改变与衰弱状态相关的死亡风险(危险比(HR,95%)P>0.05)。
衰弱状态的转变,但不是与衰弱相关的死亡风险,都受到肌少症的调节。