Family Medicine, Mayo Clinic, Rochester, Minnesota, USA
Department of Nursing, Mayo Clinic, Rochester, Minnesota, USA.
BMJ Open Qual. 2022 Jul;11(3). doi: 10.1136/bmjoq-2022-001859.
Patients with self-reported antibiotic allergies have a higher cost of care, more frequent infections with resistant bacteria and worse health outcomes than patients without antibiotic allergies. Ultimately, less than 5% of patients who report a penicillin allergy have a clinically significant immune-mediated hypersensitivity reaction when tested. As 10%-30% of the population of pregnant patients are colonised for group B (GBS) and guidelines recommend penicillin as the treatment of choice for GBS, current recommendations support penicillin allergy testing in pregnant patients who report an allergy.
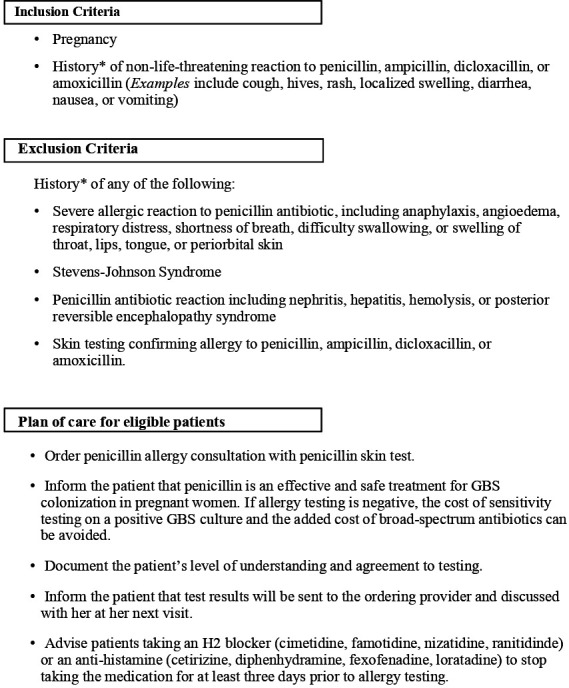
In this quality improvement project, nursing staff used an algorithm outlining inclusion and exclusion criteria to determine which patients were eligible to have penicillin allergy testing completed. Penicillin allergy testing consisted of a skin test using benzylpenicilloyl polylysine (Pre-Pen), penicillin G potassium, amoxicillin and alkaline hydrolysis mix (penicilloate) as a prick skin test, followed by intradermal skin test and finally an oral challenge with either amoxicillin or penicillin. Patient outcomes were analysed to evaluate the impact of the intervention.
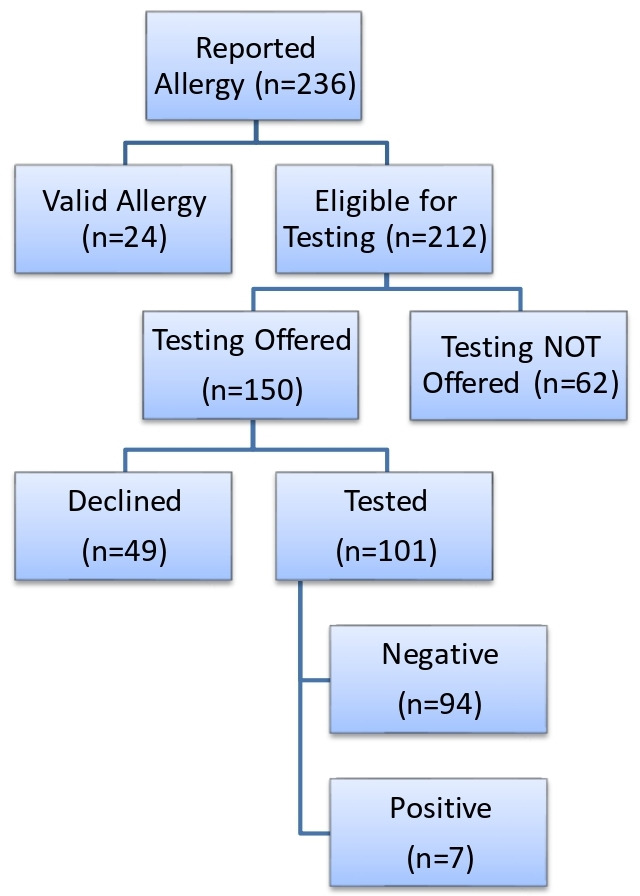
Of the 1266 patients receiving prenatal care during the intervention, 236 (19%) reported a history of penicillin allergy, and 212 if these were eligible for testing. 150 of the eligible patients were offered penicillin allergy testing. 101 patients (67%) completed testing and 49 (33%) declined testing. Seven patients (7%) had positive penicillin allergy testing, while 94 patients (93%) had negative penicillin allergy testing and were immediately de-labelled as penicillin allergic. Seventeen of the de-labelled patients subsequently tested positive for GBS colonisation, and all received intrapartum penicillin without adverse events.
Pursuing penicillin allergy testing for pregnant patients with reported penicillin allergy is a safe and feasible approach, allowing for allergy de-labelling and safe, guideline-driven antimicrobial therapy during subsequent labour and delivery hospitalisations. Cost-effectiveness of the allergy testing and impact on later episodes of care should be further investigated.
与没有抗生素过敏的患者相比,自述抗生素过敏的患者医疗费用更高,感染耐药菌的频率更高,健康状况更差。最终,当经过测试时,报告青霉素过敏的患者中只有不到 5%存在临床意义的免疫介导的过敏反应。由于 10%-30%的孕妇患者定植了 B 组链球菌(GBS),且指南建议青霉素为 GBS 的首选治疗药物,因此目前的建议支持对报告过敏的孕妇患者进行青霉素过敏测试。
在这个质量改进项目中,护理人员使用了一个算法,该算法概述了纳入和排除标准,以确定哪些患者有资格完成青霉素过敏测试。青霉素过敏测试包括使用苄青霉素酰多聚赖氨酸(Pre-Pen)、青霉素 G 钾、阿莫西林和碱性水解混合物(青霉素酸盐)进行皮试,然后进行皮内皮肤测试,最后口服阿莫西林或青霉素进行口服挑战。分析患者结局以评估干预措施的效果。
在干预期间,接受产前护理的 1266 名患者中,有 236 名(19%)报告有青霉素过敏史,如果这些患者有资格进行测试,则有 212 名。150 名符合条件的患者接受了青霉素过敏测试。101 名患者(67%)完成了测试,49 名(33%)拒绝了测试。7 名患者(7%)青霉素过敏测试呈阳性,而 94 名患者(93%)青霉素过敏测试呈阴性,立即被标记为青霉素过敏。随后,17 名被标记的患者被检测出 GBS 定植阳性,所有患者均在产程中接受了无不良反应的青霉素治疗。
对报告青霉素过敏的孕妇患者进行青霉素过敏测试是一种安全可行的方法,可进行过敏标记消除,并在随后的分娩和住院期间安全、符合指南的使用抗生素治疗。应进一步调查过敏测试的成本效益及其对后续治疗的影响。