Department of Nephropathy, Lianyungang TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Lianyungang, Jiangsu 222000, China.
Department of Emergency, Lianyungang TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Lianyungang, Jiangsu 222000, China.
Comput Math Methods Med. 2022 Jul 21;2022:4586458. doi: 10.1155/2022/4586458. eCollection 2022.
In clinical practise, it can be challenging to tell the difference between asthma and chronic obstructive pulmonary disease (COPD) and heart failure (HF), which share comparable dyspnea symptoms. We aimed to examine whether renal function indexes blood urea nitrogen (BUN), creatinine (Cr), and the ratio of BUN to Cr (BUN/Cr) can be used to distinguish HF from asthma and COPD.
A total of 170 patients were admitted for dyspnea symptoms in this retrospective study. There are 69 patients with HF (HF group), 50 patients with asthma (asthma group), and 51 patients diagnosed with COPD (COPD group). The levels of BUN, Cr, and the ratio of BUN/Cr in the three groups were compared. Student's -test or the one-way analysis of variance (ANOVA) test was used to compare means. Using the area under the receiver operating characteristic curve, model differentiation was evaluated (AUC). -test comparisons of AUC were carried out.
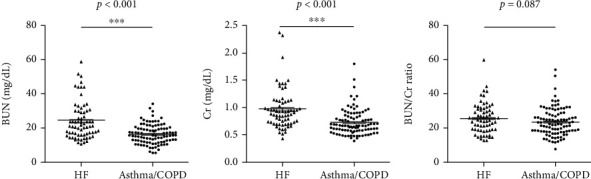
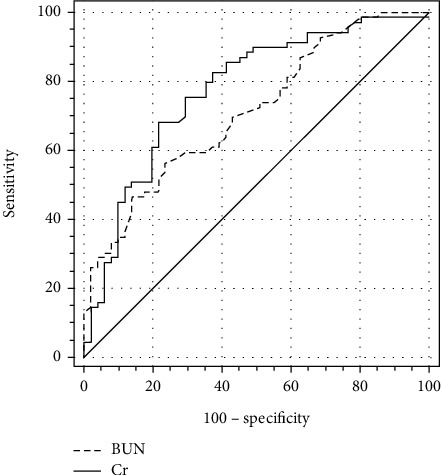
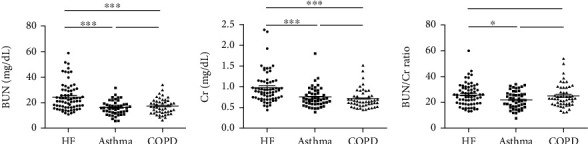
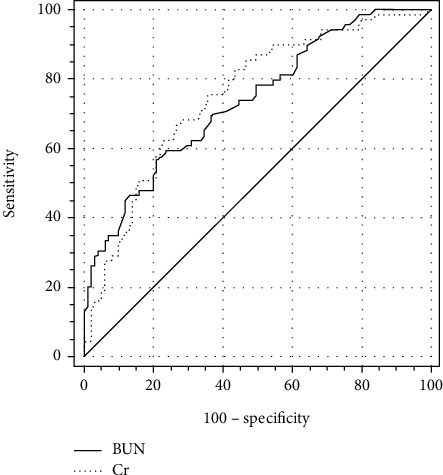
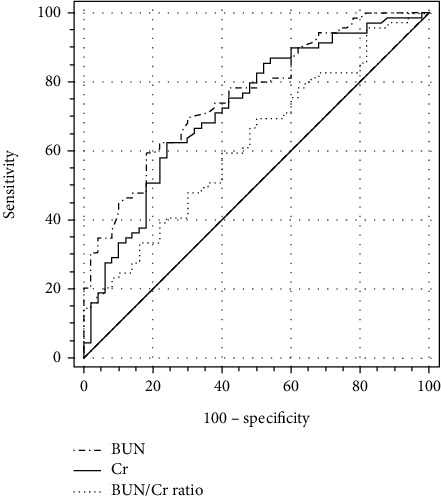
Compared with the asthma/COPD group (asthma group + COPD group) or the COPD group, the levels of BUN and Cr were raised in the HF group, while there was no significant difference of the BUN/Cr ratio. Compared with those in the asthma group, the levels of BUN, Cr, and BUN/Cr ratio were significantly increased in the HF group (all < 0.05), whereas no significant differences of BUN, Cr, and BUN/Cr ratio were found between asthma and COPD. The AUC in distinguishing HF from asthma/COPD were 0.736 and 0.751 for BUN and Cr, respectively, and no significant difference was observed between BUN and Cr. The cutoff values (specificity, sensitivity, and Youden index) in distinguishing between HF and asthma/COPD were 20.45 mg/dL (79.21%, 56.52%, and 0.357) for BUN and 0.782 mg/dL (72.28%, 68.12%, and 0.404) for Cr, respectively.
BUN and Cr showed accurate and reliable diagnostic values which could be potential biomarkers for differentiating HF from asthma and/or COPD.
在临床实践中,很难区分哮喘、慢性阻塞性肺疾病(COPD)和心力衰竭(HF),这些疾病都有类似的呼吸困难症状。我们旨在研究肾功能指标血尿素氮(BUN)、肌酐(Cr)和 BUN 与 Cr 的比值(BUN/Cr)是否可用于区分 HF 与哮喘和 COPD。
本回顾性研究共纳入 170 例因呼吸困难就诊的患者。其中 HF 患者 69 例(HF 组),哮喘患者 50 例(哮喘组),COPD 患者 51 例(COPD 组)。比较三组患者的 BUN、Cr 及 BUN/Cr 水平。采用 Student's -test 或单因素方差分析(ANOVA)检验进行均值比较。采用受试者工作特征曲线下面积(AUC)评价模型的区分度。采用 -test 比较 AUC。
与哮喘/COPD 组(哮喘组+COPD 组)或 COPD 组相比,HF 组 BUN 和 Cr 水平升高,而 BUN/Cr 比值无显著差异。与哮喘组相比,HF 组 BUN、Cr 及 BUN/Cr 比值均显著升高(均<0.05),而哮喘组与 COPD 组之间 BUN、Cr 及 BUN/Cr 比值无显著差异。BUN 和 Cr 鉴别 HF 与哮喘/COPD 的 AUC 分别为 0.736 和 0.751,两者间无显著差异。鉴别 HF 与哮喘/COPD 的最佳截断值(特异度、敏感度和约登指数)分别为 20.45mg/dL(79.21%、56.52%和 0.357)的 BUN 和 0.782mg/dL(72.28%、68.12%和 0.404)的 Cr。
BUN 和 Cr 具有准确可靠的诊断价值,可能是鉴别 HF 与哮喘和/或 COPD 的潜在生物标志物。