Agoti Charles N, Curran Martin D, Murunga Nickson, Ngari Moses, Muthumbi Esther, Lambisia Arnold W, Frost Simon D W, Blacklaws Barbara A, Nokes D James, Drumright Lydia N
Epidemiology and Demography Department, Kenya Medical Research Institute (KEMRI)-Wellcome Trust Research Programme, P.O. Box 230, Kilifi, 80108, Kenya.
School of Health and Human Sciences, Pwani University, Kilifi, Kenya.
Gut Pathog. 2022 Aug 1;14(1):32. doi: 10.1186/s13099-022-00506-z.
Kenya introduced Rotarix (GlaxoSmithKline Biologicals, Rixensart, Belgium) vaccination into its national immunization programme beginning July 2014. The impact of this vaccination program on the local epidemiology of various known enteropathogens is not fully understood.
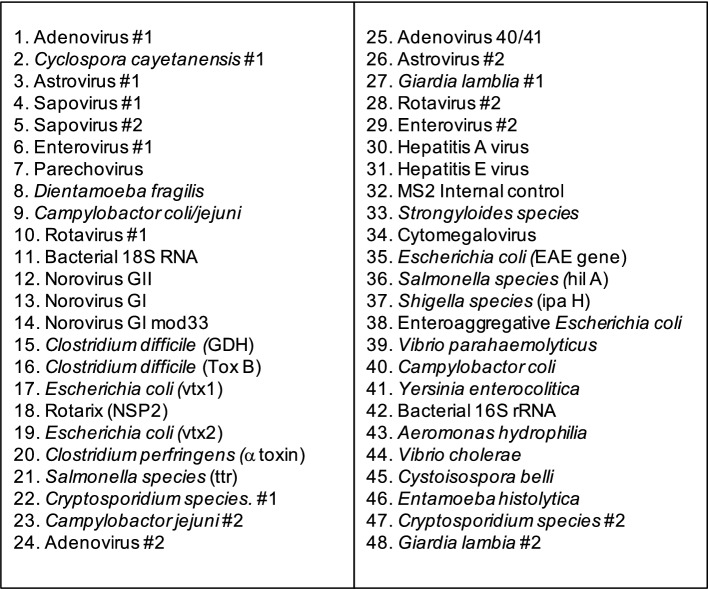
We used a custom TaqMan Array Card (TAC) to screen for 28 different enteropathogens in 718 stools from children aged less than 13 years admitted to Kilifi County Hospital, coastal Kenya, following presentation with diarrhea in 2013 (before vaccine introduction) and in 2016-2018 (after vaccine introduction). Pathogen positivity rate differences between pre- and post-Rotarix vaccination introduction were examined using both univariate and multivariable logistic regression models.
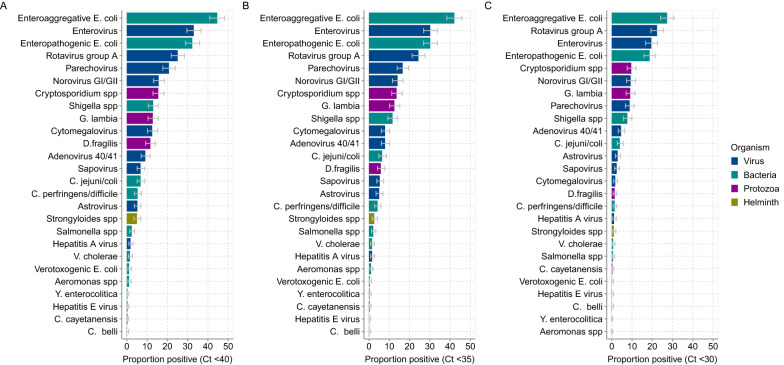
In 665 specimens (92.6%), one or more enteropathogen was detected, while in 323 specimens (48.6%) three or more enteropathogens were detected. The top six detected enteropathogens were: enteroaggregative Escherichia coli (EAggEC; 42.1%), enteropathogenic Escherichia coli (EPEC; 30.2%), enterovirus (26.9%), rotavirus group A (RVA; 24.8%), parechovirus (16.6%) and norovirus GI/GII (14.4%). Post-rotavirus vaccine introduction, there was a significant increase in the proportion of samples testing positive for EAggEC (35.7% vs. 45.3%, p = 0.014), cytomegalovirus (4.2% vs. 9.9%, p = 0.008), Vibrio cholerae (0.0% vs. 2.3%, p = 0.019), Strongyloides species (0.8% vs. 3.6%, p = 0.048) and Dientamoeba fragilis (2.1% vs. 7.8%, p = 0.004). Although not reaching statistical significance, the positivity rate of adenovirus 40/41 (5.8% vs. 7.3%, p = 0.444), norovirus GI/GII (11.2% vs. 15.9%, p = 0.089), Shigella species (8.7% vs. 13.0%, p = 0.092) and Cryptosporidium spp. (11.6% vs. 14.7%, p = 0.261) appeared to increase post-vaccine introduction. Conversely, the positivity rate of sapovirus decreased significantly post-vaccine introduction (7.8% vs. 4.0%, p = 0.030) while that of RVA appeared not to change (27.4% vs. 23.5%, p = 0.253). More enteropathogen coinfections were detected per child post-vaccine introduction compared to before (mean: 2.7 vs. 2.3; p = 0.0025).
In this rural Coastal Kenya setting, childhood enteropathogen infection burden was high both pre- and post-rotavirus vaccination introduction. Children who had diarrheal admissions post-vaccination showed an increase in coinfections and changes in specific enteropathogen positivity rates. This study highlights the utility of multipathogen detection platforms such as TAC in understanding etiology of childhood acute gastroenteritis in resource-limited regions.
肯尼亚自2014年7月起将Rotarix疫苗(葛兰素史克生物制品公司,比利时里克森堡)纳入其国家免疫规划。该疫苗接种计划对当地各种已知肠道病原体流行病学的影响尚未完全了解。
我们使用定制的TaqMan Array Card(TAC)对肯尼亚沿海基利菲县医院收治的718例13岁以下腹泻儿童的粪便样本进行检测,筛查28种不同的肠道病原体,这些样本分别采集于2013年(疫苗引入前)和2016 - 2018年(疫苗引入后)。采用单变量和多变量逻辑回归模型检验Rotarix疫苗引入前后病原体阳性率的差异。
在665份样本(92.6%)中检测到一种或多种肠道病原体,在323份样本(48.6%)中检测到三种或更多种肠道病原体。检测到的前六种肠道病原体为:肠集聚性大肠杆菌(EAggEC;42.1%)、肠致病性大肠杆菌(EPEC;30.2%)、肠道病毒(26.9%)、A组轮状病毒(RVA;24.8%)、细小病毒(16.6%)和诺如病毒GI/GII(14.4%)。引入轮状病毒疫苗后,EAggEC检测阳性样本比例显著增加(35.7%对45.3%,p = 0.014),巨细胞病毒(4.2%对9.9%,p = 0.008)、霍乱弧菌(0.0%对2.3%,p = 0.019)、类圆线虫属(0.8%对3.6%,p = 0.048)和脆弱双核阿米巴(2.1%对7.8%,p = 0.004)。虽然未达到统计学显著性,但疫苗引入后腺病毒40/41(5.8%对7.3%,p = 0.444)、诺如病毒GI/GII(11.2%对15.9%,p = 0.089)、志贺菌属(8.7%对13.0%,p = 0.092)和隐孢子虫属(11.6%对14.7%,p = 0.261)的阳性率似乎有所增加。相反,疫苗引入后札幌病毒的阳性率显著下降(7.8%对4.0%,p = 0.030),而RVA的阳性率似乎没有变化(27.4%对23.5%,p = 0.253)。与疫苗引入前相比,疫苗引入后每个儿童检测到的肠道病原体合并感染更多(平均值:2.7对2.3;p = 0.0025)。
在肯尼亚沿海这个农村地区,轮状病毒疫苗引入前后儿童肠道病原体感染负担都很高。接种疫苗后因腹泻入院的儿童合并感染增加,特定肠道病原体阳性率发生了变化。本研究强调了TAC等多病原体检测平台在了解资源有限地区儿童急性胃肠炎病因方面的作用。