School of Medicine, Virginia Commonwealth University, Richmond, VA, USA.
Department of Surgery, Hunter Holmes McGuire VA Medical Center, Richmond, VA, USA.
Am J Case Rep. 2022 Aug 2;23:e937197. doi: 10.12659/AJCR.937197.
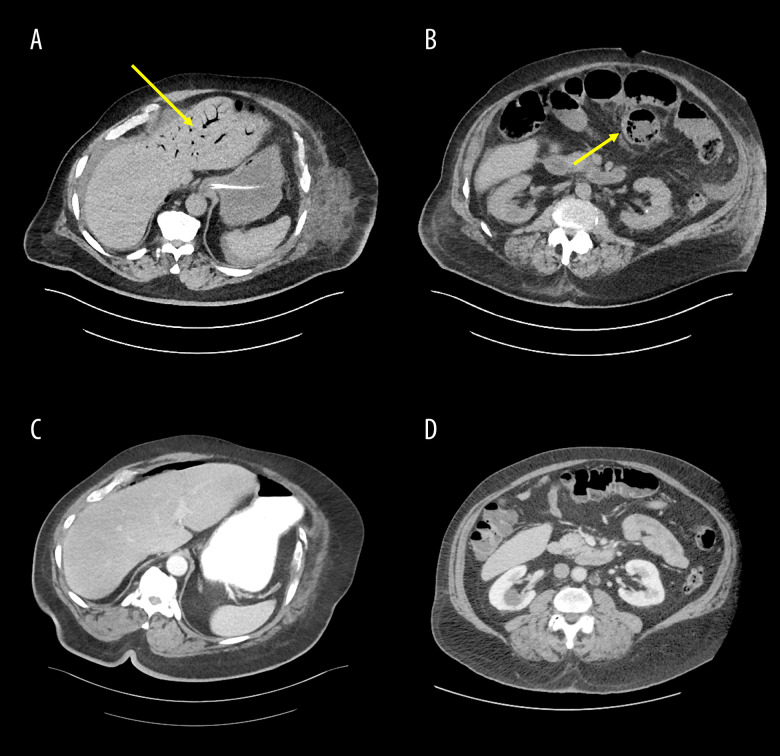
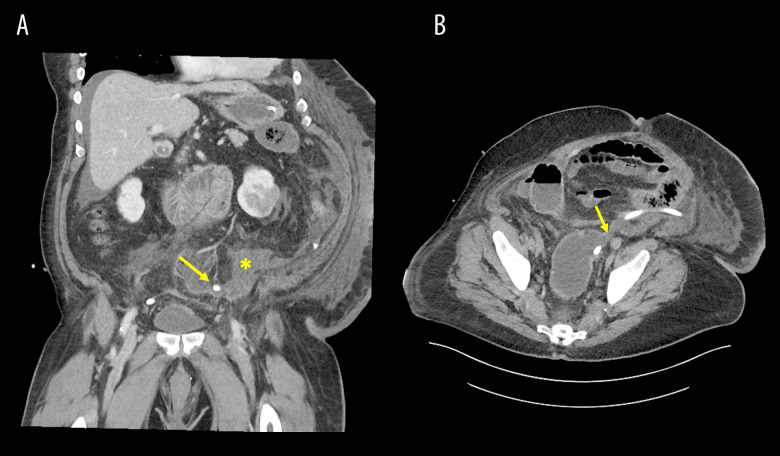
BACKGROUND Hepatic portal venous gas is a rare and concerning finding occasionally seen on computed tomography (CT) scans, and must be emergently managed, often in the operating room. This condition can present in conjunction with bowel distension, pneumatosis intestinalis, and intestinal ischemia, so care must be taken to examine the imaging closely so as not to miss this dire condition. This report summarizes our experience with a patient who had this problem and how urgent management prevented a lethal outcome. CASE REPORT The patient was a 77-year-old morbidly obese man whose complicated hospital course began with admission for abdominal pain evaluation. This led to a flexible sigmoidoscopy for concerning CT findings suggestive of colitis or malignancy, leading to a perforation at the anterior wall of the sigmoid-rectal junction. Urgent sigmoid colectomy and Hartmann's procedure were performed along with pelvic drainage. Blood cultures returned positive for Klebsiella. After 10 days, the patient decompensated, and a CT scan showed pneumatosis intestinalis, hepatic portal venous gas, and diffuse small bowel distension. Rectal stump dehiscence had occurred; therefore, 2 repeat abdominal wash-outs were performed with aggressive intensive care. The patient eventually stabilized and was ultimately discharged to a skilled nursing facility 32 days later. CONCLUSIONS This case illustrates the importance of prompt imaging, medical management, and, if necessary, surgical exploration in the patient with bowel distension and hepatic portal venous gas on a CT scan. Although uncommon, this finding indicates a potentially poor prognosis and must be addressed emergently to prevent bowel ischemia from progressing in patients with underlying abdominal pathology.
肝门静脉积气是一种罕见且令人担忧的 CT 扫描结果,必须紧急处理,通常在手术室进行。这种情况可能与肠扩张、肠气肿和肠缺血同时出现,因此必须仔细检查影像学结果,以免漏诊这种危急情况。本报告总结了我们对一位患有此问题的患者的经验,以及紧急处理如何防止致命结局。
患者为 77 岁病态肥胖男性,其复杂的住院过程始于腹痛评估。这导致了直肠乙状结肠镜检查,因为 CT 发现有结肠炎或恶性肿瘤的可疑表现,导致乙状结肠直肠交界处前壁穿孔。紧急进行了乙状结肠切除术和 Hartmann 手术,并进行了盆腔引流。血培养结果显示为克雷伯氏菌阳性。10 天后,患者失代偿,CT 扫描显示肠气肿、肝门静脉积气和弥漫性小肠扩张。直肠残端裂开;因此,进行了 2 次重复的腹腔冲洗和积极的重症监护。患者最终稳定下来,并在 32 天后出院到专业护理机构。
本病例说明了在 CT 扫描显示肠扩张和肝门静脉积气的患者中,及时进行影像学检查、内科治疗和必要时手术探查的重要性。尽管这种情况并不常见,但这种发现表明预后可能较差,必须紧急处理,以防止潜在的腹部病理患者的肠缺血进展。