Department of Urology, Tulane University School of Medicine, New Orleans, LA, USA.
Southeast Louisiana Veterans Health Care System, New Orleans, LA, USA.
Oncologist. 2023 Feb 8;28(2):149-156. doi: 10.1093/oncolo/oyac154.
This study aimed to evaluate if race impacted outcomes or risk of disease progression in men on active surveillance (AS) for prostate cancer. We present the results from our majority African-American cohort of men in an equal access setting over a 5-year follow-up period.
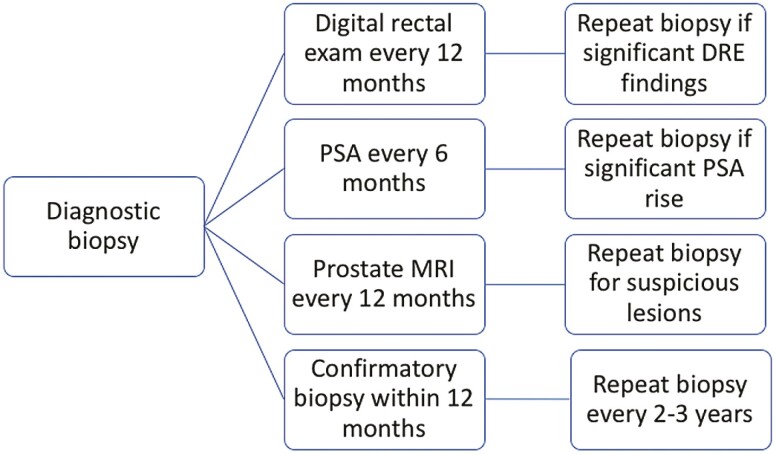
All patients who elected AS for prostate cancer at the Southeast Louisiana Veterans Health Care System are entered into a prospectively managed observational database. Patients were divided into groups based on self-reported race. Grade group progression was defined as pathologic upgrading above International Society of Urological Pathology Grade Group 1 disease on subsequent biopsies following diagnostic biopsy. All tests were 2 sided using a significance of .05.
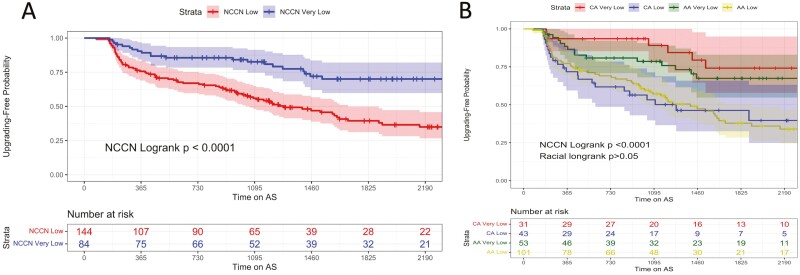
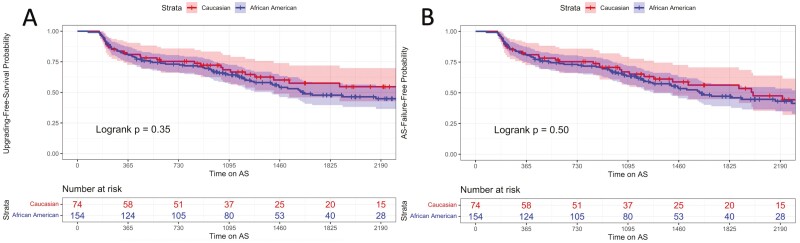
A total of 228 men met inclusion criteria in the study, including 154 non-Hispanic African American and 74 non-Hispanic Caucasian American men, with a median follow-up of 5 years from the initiation of AS. Race was not predictive of Gleason grade progression, AS discontinuation, or biochemical recurrence on Cox multivariate analysis (HR = 1.01, 0.94, 0.85, P = .96, .79, .81, respectively). On Kaplan-Meier analysis at 5 years, African-American progression-free, AS discontinuation free, and overall survival probability was comparable to their Caucasian American counterparts (P > .05 for all).
Active surveillance is a safe treatment option for low and very low risk prostate cancer, regardless of race. African-American and Caucasian-American men did not have any significant difference in Gleason grade group progression in our cohort with 5-year follow-up.
本研究旨在评估在接受前列腺癌主动监测(AS)的男性中,种族是否会影响结局或疾病进展的风险。我们呈现了在一个平等获得医疗资源的环境下,对我们的以非裔美国人为主的队列的研究结果,随访时间为 5 年。
所有在路易斯安那州东南部退伍军人医疗保健系统选择 AS 治疗前列腺癌的患者都被纳入前瞻性管理的观察性数据库。患者根据自我报告的种族分为不同的组。分级分组进展定义为在诊断性活检后后续活检中出现国际泌尿病理学会分级分组 1 以上的病理性升级。所有检验均为双侧检验,显著性水平为.05。
本研究共纳入 228 名符合条件的男性患者,包括 154 名非西班牙裔非洲裔美国人和 74 名非西班牙裔白种人,从开始 AS 到中位随访 5 年。在 Cox 多变量分析中,种族不能预测 Gleason 分级进展、AS 终止或生化复发(HR = 1.01、0.94、0.85,P =.96、.79、.81)。在 Kaplan-Meier 分析中,5 年时非裔美国人的无进展生存、AS 无终止生存和总生存概率与他们的白种人对照组相当(所有 P >.05)。
主动监测是低危和极低危前列腺癌的安全治疗选择,与种族无关。在我们的队列中,随访 5 年,非裔美国人和白种人在 Gleason 分级分组进展方面没有显著差异。