London School of Hygiene and Tropical Medicine, London, UK, UK.
UK Severe Asthma Network and National Registry, Queen's University Belfast, Belfast, UK.
Thorax. 2023 Jul;78(7):643-652. doi: 10.1136/thorax-2021-217032. Epub 2022 Aug 3.
Progressive lung function (LF) decline in patients with asthma contributes to worse outcomes. Asthma exacerbations are thought to contribute to this decline; however, evidence is limited with mixed results.
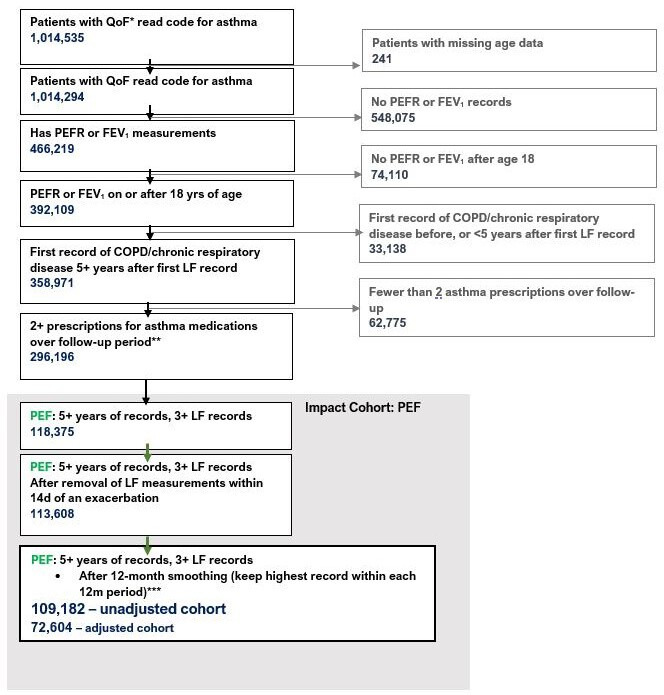
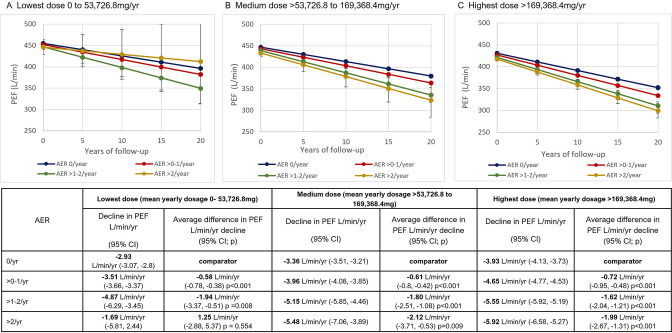
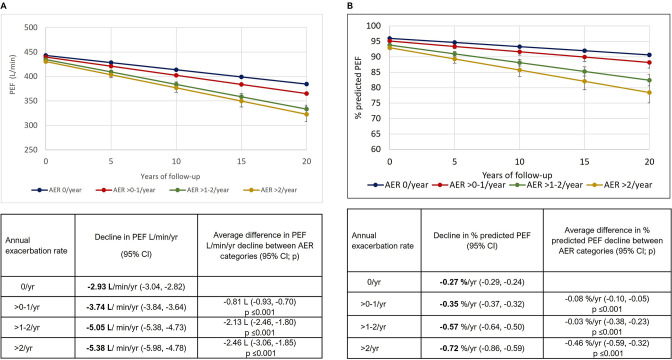
This historical cohort study of a broad asthma patient population in the Optimum Patient Care Research Database, examined asthma patients with 3+eligible post-18th birthday peak expiratory flow rate (PEF) records (primary analysis) or records of forced expiratory flow in 1 s (FEV) (sensitivity analysis). Adjusted linear growth models tested the association between mean annual exacerbation rate (AER) and LF trajectory.
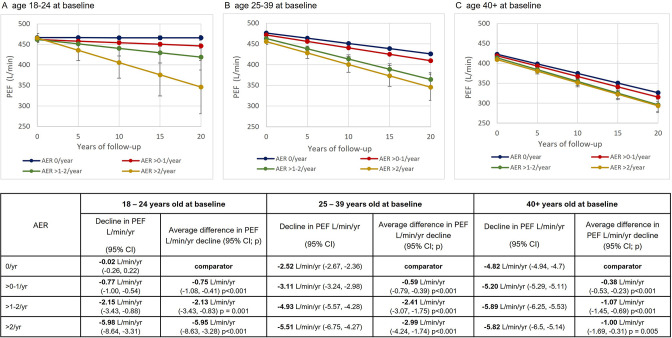
We studied 1 09 182 patients with follow-up ranging from 5 to 50 years, of which 75 280 had data for all variables included in the adjusted analyses. For each additional exacerbation, an estimated additional -1.34 L/min PEF per year (95% CI -1.23 to -1.50) were lost. Patients with AERs >2/year and aged 18-24 years at baseline lost an additional -5.95 L/min PEF/year (95% CI -8.63 to -3.28) compared with those with AER 0. These differences in the rate of LF decline between AER groups became progressively smaller as age at baseline increased. The results using FEV were consistent with the above.
To our knowledge, this study is the largest nationwide cohort of its kind and demonstrates that asthma exacerbations are associated with faster LF decline. This was more prominent in younger patients but was evident in older patients when it was related to lower starting LF, suggesting a persistent deteriorating phenotype that develops in adulthood over time. Earlier intervention with appropriate management in younger patients with asthma could be of value to prevent excessive LF decline.
哮喘患者的肺功能(LF)逐渐下降会导致预后更差。哮喘加重被认为是导致这种下降的原因,但证据有限且结果不一。
本研究通过 Optimum Patient Care Research Database 中的一个广泛的哮喘患者人群的历史队列研究,对 3 岁及以上有合格的呼气峰流速(PEF)记录(主要分析)或 1 秒用力呼气量(FEV)记录的哮喘患者(敏感性分析)进行了研究。调整后的线性增长模型检验了平均每年加重率(AER)与 LF 轨迹之间的关联。
我们研究了 109182 名患者,随访时间从 5 年到 50 年不等,其中 75280 名患者具有纳入调整分析的所有变量的数据。每增加一次加重,预计每年会损失 1.34L/min 的 PEF(95%CI-1.23 至-1.50)。与 AER 为 0 的患者相比,基线年龄为 18-24 岁且 AER >2/年的患者每年会额外损失 5.95L/min 的 PEF(95%CI-8.63 至-3.28)。与 AER 组之间 LF 下降率的这些差异随着基线年龄的增加而逐渐减小。使用 FEV 的结果与上述结果一致。
据我们所知,这是此类研究中规模最大的全国性队列研究,表明哮喘加重与 LF 下降较快有关。在年轻患者中更为明显,但在与较低的起始 LF 相关的老年患者中也很明显,这表明随着时间的推移,一种在成年后逐渐发展的持续恶化的表型。在年轻哮喘患者中尽早进行适当的管理干预可能有助于防止 LF 过度下降。