Cremer Paul C, Sheng Calvin C, Sahoo Debasis, Dugar Siddharth, Prada Robier Aguillon, Wang Tom Kai Ming, Hassan Ossama K Abou, Hernandez-Montfort Jamie, Wolinsky David A, Culver Daniel A, Rajendram Prabalini, Duggal Abhijit, Brennan Danielle M, Wolski Katherine E, Lincoff A Michael, Nissen Steven E, Menon Venu
Department of Cardiovascular Medicine, Heart, Vascular and Thoracic Institute, Cleveland Clinic, Cleveland, OH, USA.
Department of Pulmonary Medicine, Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA.
Eur Heart J Open. 2021 Jul 29;1(1):oeab002. doi: 10.1093/ehjopen/oeab002. eCollection 2021 Aug.
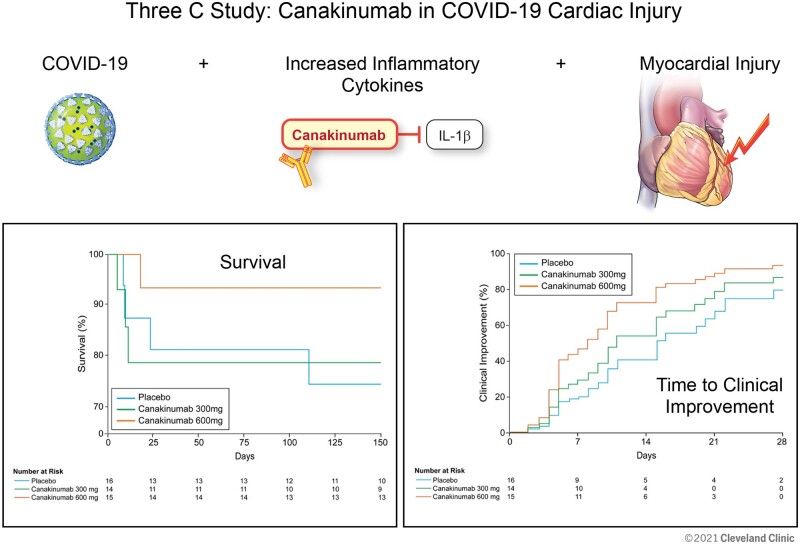
In coronavirus disease 2019 (COVID-19), myocardial injury is associated with systemic inflammation and higher mortality. Our aim was to perform a proof of concept trial with canakinumab, a monoclonal antibody to interleukin-1β, in patients with COVID-19, myocardial injury, and heightened inflammation.
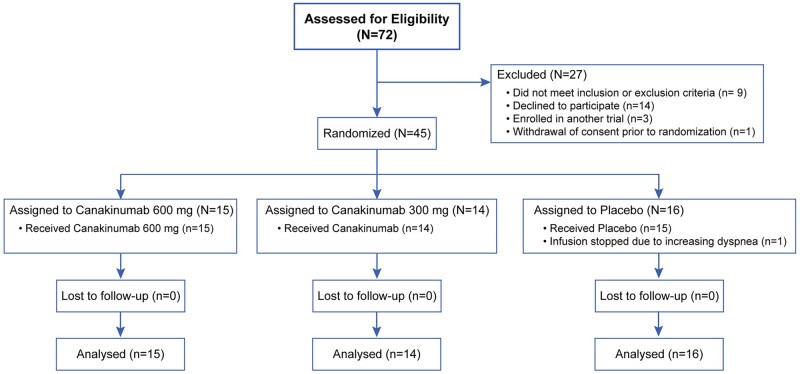
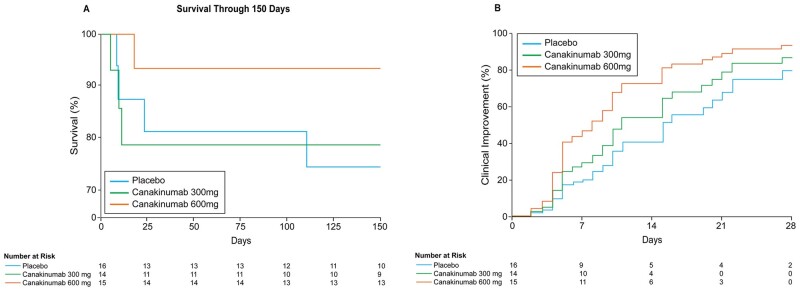
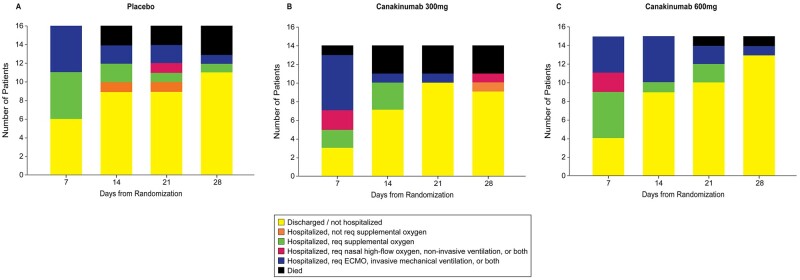
This trial required hospitalization due to COVID-19, elevated troponin, and a C-reactive protein concentration more than 50 mg/L. The primary endpoint was time to clinical improvement at Day 14, defined as either an improvement of two points on a seven-category ordinal scale or discharge from the hospital. The secondary endpoint was mortality at Day 28. Forty-five patients were randomly assigned to canakinumab 600 mg ( = 15), canakinumab 300 mg ( = 14), or placebo ( = 16). There was no difference in time to clinical improvement compared to placebo [recovery rate ratio (RRR) for canakinumab 600 mg 1.15, 95% confidence interval (CI) 0.46-2.91; RRR for canakinumab 300 mg 0.61, 95% CI 0.23-1.64]. At Day 28, 3 (18.8%) of 15 patients had died in the placebo group, compared with 3 (21.4%) of 14 patients with 300 mg canakinumab, and 1 (6.7%) of 15 patients with 600 mg canakinumab. There were no treatment-related deaths, and adverse events were similar between groups.
There was no difference in time to clinical improvement at Day 14 in patients treated with canakinumab, and no safety concerns were identified. Future studies could focus on high dose canakinumab in the treatment arm and assess efficacy outcomes at Day 28.
在2019冠状病毒病(COVID-19)中,心肌损伤与全身炎症及更高的死亡率相关。我们的目的是在患有COVID-19、心肌损伤且炎症加剧的患者中进行一项使用抗白细胞介素-1β单克隆抗体卡那单抗的概念验证试验。
该试验要求患者因COVID-19住院、肌钙蛋白升高且C反应蛋白浓度超过50mg/L。主要终点是第14天临床改善的时间,定义为在七分类序贯量表上改善两分或出院。次要终点是第28天的死亡率。45名患者被随机分配至卡那单抗600mg组(n = 15)、卡那单抗300mg组(n = 14)或安慰剂组(n = 16)。与安慰剂相比,临床改善时间无差异[卡那单抗600mg组的恢复率比(RRR)为1.15,95%置信区间(CI)为0.46 - 2.91;卡那单抗300mg组的RRR为0.61,95%CI为0.23 - 1.64]。在第28天,安慰剂组15名患者中有3名(18.8%)死亡,卡那单抗300mg组14名患者中有3名(21.4%)死亡,卡那单抗600mg组15名患者中有1名(6.7%)死亡。无治疗相关死亡,且各组不良事件相似。
接受卡那单抗治疗的患者在第14天临床改善时间无差异,且未发现安全问题。未来研究可聚焦于治疗组中的高剂量卡那单抗,并评估第28天的疗效结果。