School of Nursing, University of Minnesota, Minneapolis, Minnesota, USA.
Department of Biostatistics, Yale Center for Analytical Sciences, Yale School of Public Health, New Haven, Connecticut, USA.
J Am Geriatr Soc. 2022 Nov;70(11):3116-3126. doi: 10.1111/jgs.17983. Epub 2022 Aug 4.
Evidence-based multifactorial fall prevention interventions in clinical practice have been less effective than expected. One plausible reason is that older adults' engagement in fall prevention care is suboptimal.
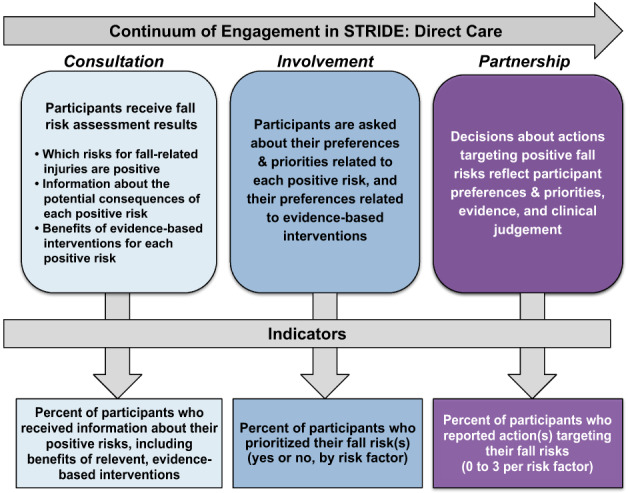
This was a post-hoc analysis of 2403 older adults' engagement in a multifactorial fall prevention intervention in the Strategies to Reduce Injuries and Develop Confidence in Elders (STRIDE) pragmatic trial. Based on the direct clinical care level of the Patient and Family Continuum of Engagement (CE) framework, three indicators of progressively interactive engagement were assessed: (1) Consultation (receiving information), (2) Involvement (prioritizing risks), and (3) Partnership (identifying prevention actions). Drop off at each step was determined as well as predictors of engagement.
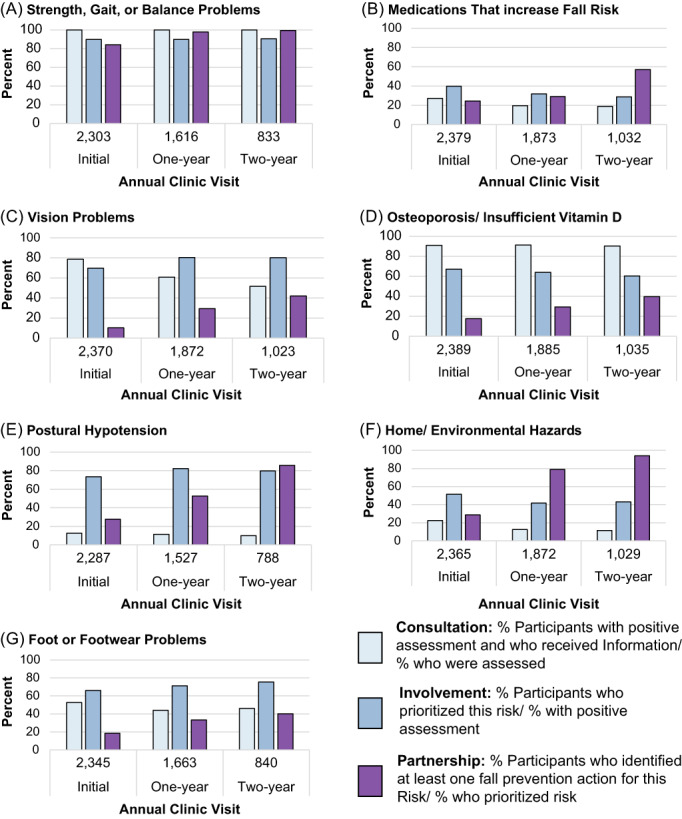
The participants' engagement waned with increasingly interactive CE domains. Although all participants received information about their positive fall risk factors (consultation) and most (51%-96%) prioritized them (involvement), fewer participants (33%-55%) identified fall prevention actions (partnership) for most of their risk factors, except for strength gait or balance problems (95%). More participants (70%) identified home exercises than other actions. Finally, fall prevention actions were identified more commonly among participants who received two visits compared to one (OR = 2.33 [95% CI, 2.06-2.64]), were ≥80 years old (OR = 1.83 [95% CI, 1.51-2.23]), and had fewer fall risk factors (OR = 0.90 [95% CI, 0.83-0.99]).
The drop-off in participants' engagement based on the level of their interaction with clinicians suggests that future multifactorial fall prevention interventions need to be more focused on interactive patient-clinician partnerships that help older adults increase and maintain fall prevention actions. Our analyses suggest that more frequent contact with clinicians and more monitoring of the implementation and outcomes of Fall Prevention Care Plans could potentially improve engagement and help older adults maintain fall prevention actions.
在临床实践中,基于证据的多因素防跌倒干预措施的效果不如预期。一个合理的原因是,老年人参与防跌倒护理的程度不理想。
这是对 2403 名老年人参与 STRIDE 实用性试验中的多因素防跌倒干预措施的后续分析。基于患者和家庭参与连续性(CE)框架的直接临床护理水平,评估了三个渐进式互动参与指标:(1)咨询(接受信息)、(2)参与(确定风险优先级)和(3)合作(确定预防措施)。确定了每个步骤的脱落情况以及参与的预测因素。
参与者的参与程度随着 CE 领域的互动性增加而减弱。尽管所有参与者都收到了有关其积极跌倒风险因素的信息(咨询),并且大多数人(51%-96%)将其作为优先事项(参与),但只有较少的参与者(33%-55%)为大多数风险因素确定了防跌倒措施(合作),除了力量、步态或平衡问题(95%)。与其他行动相比,更多的参与者(70%)确定了家庭锻炼。最后,与接受一次就诊相比,接受两次就诊的参与者更常见地确定了防跌倒措施(OR=2.33[95%CI,2.06-2.64]),年龄≥80 岁(OR=1.83[95%CI,1.51-2.23]),并且跌倒风险因素较少(OR=0.90[95%CI,0.83-0.99])。
根据参与者与临床医生互动水平的参与度下降表明,未来的多因素防跌倒干预措施需要更加注重互动的医患合作关系,帮助老年人增加和维持防跌倒措施。我们的分析表明,更频繁地与临床医生接触以及更频繁地监测防跌倒护理计划的实施和结果,可能会提高参与度并帮助老年人维持防跌倒措施。