Clinical Research Division, Fred Hutchinson Cancer Center, Seattle, WA, USA; Department of Medicine, Division of Hematology/Oncology, University of Washington, Seattle, WA, USA; Maladies du Sang, CHU d'Angers, Angers, France; Fédération Hospitalo-Universitaire Grand-Ouest Acute Leukemia, FHU-GOAL; Université d'Angers, Inserm UMR 1307, CNRS UMR 6075, Nantes Université, CRCI2NA, F-49000 Angers.
Cytogenetics Laboratory, Fred Hutchinson Cancer Center, Seattle, WA.
Haematologica. 2023 Feb 1;108(2):420-432. doi: 10.3324/haematol.2022.281585.
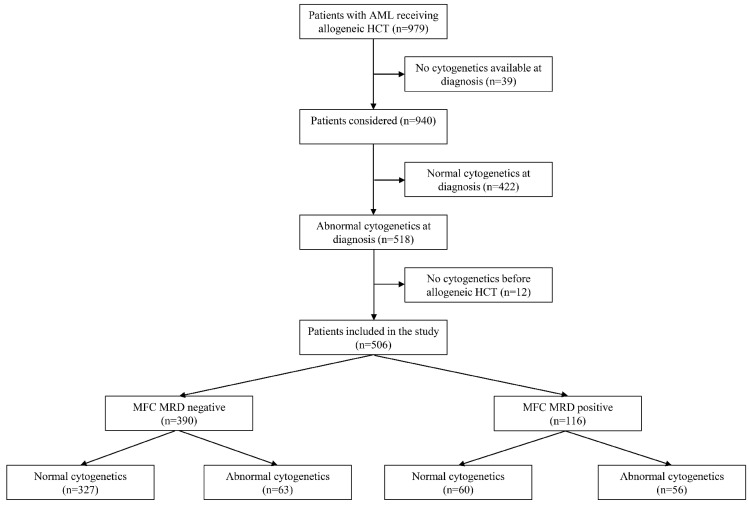
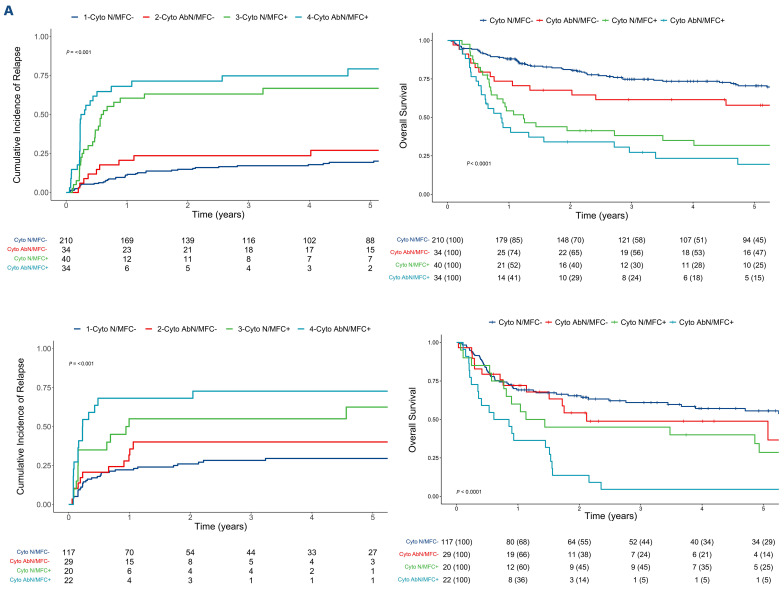
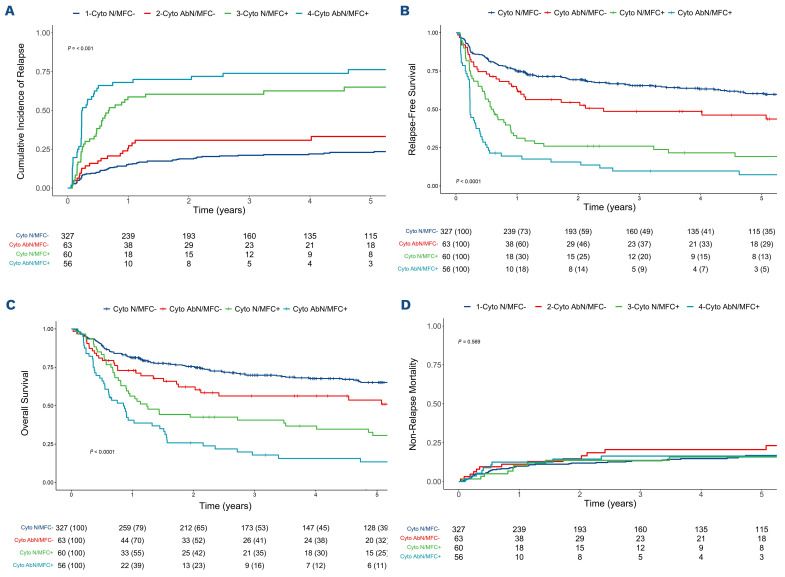
Measurable residual disease (MRD) before hematopoietic cell transplantation (HCT) is an independent established prognostic factor in patients with acute myeloid leukemia (AML). Several methods exist to evaluate the presence of residual leukemia cells, but how these are used best in combination is unclear. In order to examine how residual cytogenetic abnormalities and MRD testing by multiparameter flow cytometry (MFC) may refine risk assessment before HCT, we analyzed 506 adults with cytogenetically abnormal AML who underwent both routine karyotyping and MFC MRD testing before receiving a first allograft while in morphologic remission. Testing for residual cytogenetic abnormalities and MFC MRD identified four groups of patients with differential relapse-free survival (RFS) (hazard ratio [HR]=1.63 for Cytoabnormal/MFCnegative [P=0.01, n=63], HR=3.24 for Cytonormal/MFCpositive [P<0.001, n=60], and HR=5.50 for Cytoabnormal/MFCpositive [P<0.001, n=56] with Cytonormal/MFCnegative as reference [n=327]) and overall survival (OS) (HR=1.55 for Cytoabnormal/MFCnegative [P=0.03], HR=2.69 for Cytonormal/MFCpositive [P<0.001], and HR=4.15 for Cytoabnormal/MFCpositive [P<0.001] with Cytonormal/MFCnegative as reference). Results were similar for patients who received myeloablative or non-myeloablative conditioning. C-statistic values were higher, indicating higher accuracy, when using pre-HCT cytogenetic and MFC MRD information together for prediction of relapse, RFS, and OS, rather than using either test result alone. This study indicates that residual cytogenetic abnormalities and MFC MRD testing provide complementary prognostic information for post- HCT outcomes in patients with cytogenetically abnormal AML undergoing allogeneic HCT.
移植前造血细胞(HCT)的可测量残留疾病(MRD)是急性髓性白血病(AML)患者独立的既定预后因素。有几种方法可以评估残留白血病细胞的存在,但如何最好地结合使用这些方法尚不清楚。为了研究移植前残留细胞遗传学异常和多参数流式细胞术(MFC)MRD 检测如何改善 HCT 前的风险评估,我们分析了 506 例接受过常规核型分析和 MFC MRD 检测的细胞遗传学异常 AML 成人患者,这些患者在形态学缓解时接受了第一次同种异体移植。残留细胞遗传学异常和 MFC MRD 检测鉴定了 4 组具有不同无复发生存率(RFS)的患者(Cytoabnormal/MFCnegative 的危险比[HR]为 1.63[P=0.01,n=63],Cytonormal/MFCpositive 的 HR 为 3.24[P<0.001,n=60],Cytoabnormal/MFCpositive 的 HR 为 5.50[P<0.001,n=56],以 Cytonormal/MFCnegative 为参考[n=327])和总生存(OS)(Cytoabnormal/MFCnegative 的 HR 为 1.55[P=0.03],Cytonormal/MFCpositive 的 HR 为 2.69[P<0.001],Cytoabnormal/MFCpositive 的 HR 为 4.15[P<0.001],以 Cytonormal/MFCnegative 为参考)。在接受清髓或非清髓条件预处理的患者中,结果相似。当使用移植前细胞遗传学和 MFC MRD 信息共同预测复发、RFS 和 OS 时,C 统计值更高,表明准确性更高,而不是单独使用任何一种检测结果。这项研究表明,残留细胞遗传学异常和 MFC MRD 检测为接受异基因 HCT 的细胞遗传学异常 AML 患者的 HCT 后结局提供了互补的预后信息。