Department of Rheumatology and Clinical Immunology, Faculty of Medicine, University of Thessaly, Larissa, Greece.
Department of Neurology, Faculty of Medicine, University of Thessaly, Larissa, Greece.
Clin Exp Immunol. 2022 Oct 21;210(1):79-89. doi: 10.1093/cei/uxac069.
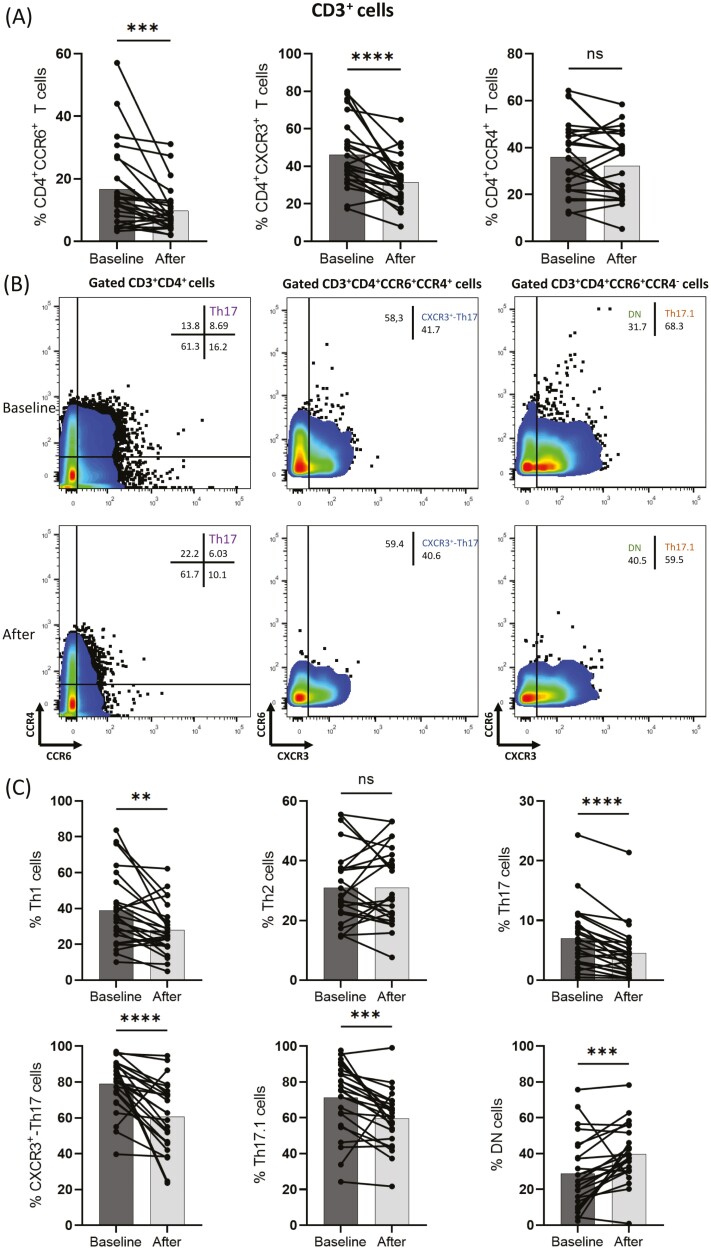
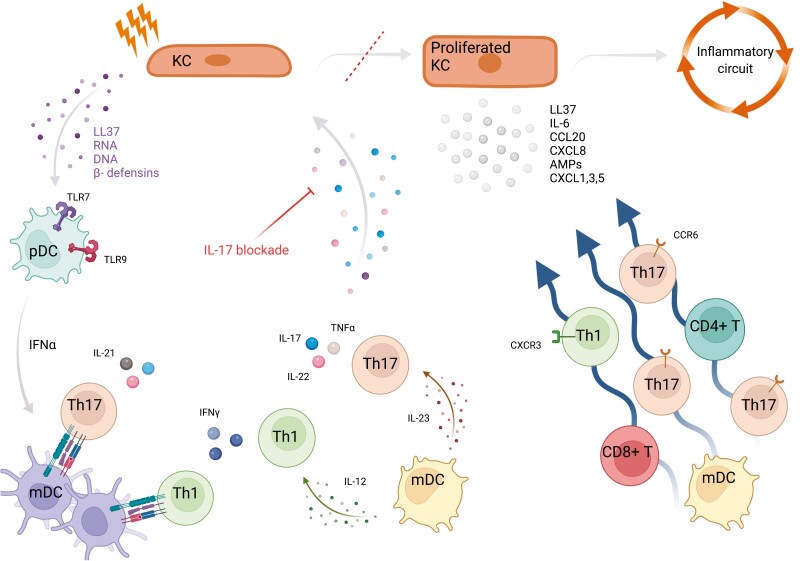
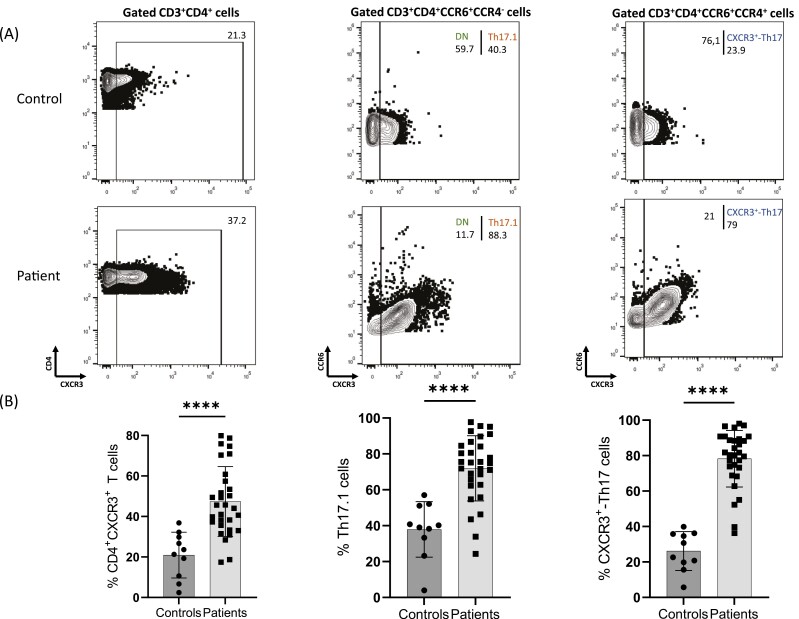
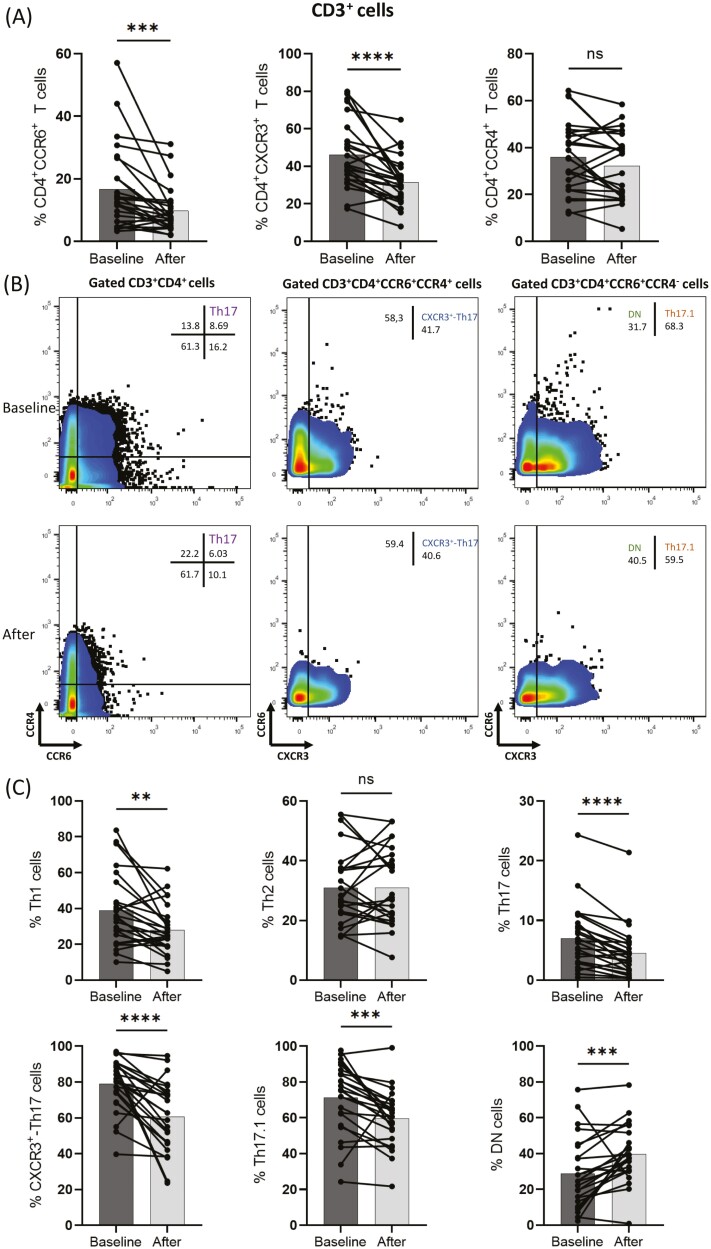
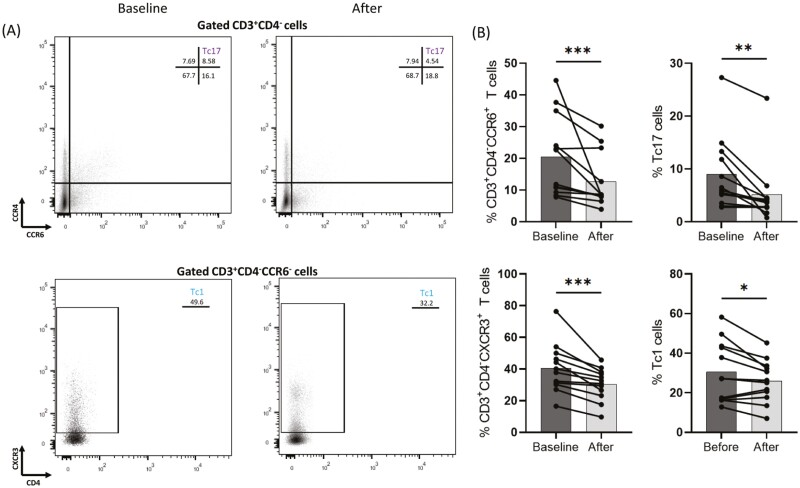
Psoriasis-an immune-mediated skin disease-implicates in its pathophysiology by circulating pro-inflammatory cell populations, cytokines, and their interactions with the epidermis. The direct effect of approved anti-interleukin- (IL-)17A and anti-IL-17R biologic therapy on immunophenotyping of peripheral blood mononuclear lymphocytes' (PBMCs) relative sub-population frequencies in psoriasis patients has not yet been described. Using multiparameter flow cytometry we examined T-cell subpopulations characterized by CCR6, CCR4, and CXCR3 chemokine receptor surface expression at baseline and after initiation of biologic therapy in PBMCs collected from 30 psoriasis patients. Increased CD3+CD4+CXCR3+, CD3+CD4+CCR6+CCR4+CXCR3+(CXCR3+-Th17), and CD3+CD4+CCR6+CCR4-CXCR3+(Th17.1) cell populations were observed in patients with psoriasis in comparison to healthy individuals (n = 10). IL-17 therapeutic blockade decreased CD3+CD4+CCR6+, CD3+CD4+CXCR3+, CD3+CD4+CCR6-CXCR3+(Th1), CD3+CD4+CCR6+CCR4+(Th17), CD3+CD4+CCR6+CCR4+CXCR3+(CXCR3+-Th17), and CD3+CD4+CCR6+CCR4-CXCR3+(Th17.1) cell populations in responding psoriasis patients. Moreover, CD3+CD4-CCR6+, CD3+CD4-CXCR3+, CD3+CD4-CCR6+CCR4+(Tc17), and CD3+CD4-CCR6-CXCR3+(Tc1) percentages were also inhibited. Modulation of the same cell sub-populations was also assessed in patients treated with methotrexate (n = 4), apremilast (n = 4), and anti-IL-23 biologic treatment (n = 4). In our study, the levels and functional capacity of peripheral pro-inflammatory Th1, Th17, and additional CCR6+T cell sub-gated populations from psoriasis patients that were treated with anti-IL-17 or anti-IL-17R targeted biologic therapy were explored for the first time. Our data clearly demonstrate that early anti-IL-17 mediated clinical remission is accompanied by a significant decrease of Th1, Th17, CXCR3+-Th17, and Th17.1 cells.
银屑病是一种免疫介导的皮肤疾病,其病理生理学涉及循环促炎细胞群、细胞因子及其与表皮的相互作用。已批准的抗白细胞介素(IL)-17A 和抗 IL-17R 生物疗法对银屑病患者外周血单个核细胞(PBMC)相对亚群频率的免疫表型的直接影响尚未描述。我们使用多参数流式细胞术检查了在 30 名银屑病患者的 PBMC 中,在开始生物治疗前后,基于 CCR6、CCR4 和 CXCR3 趋化因子受体表面表达特征的 T 细胞亚群。与健康个体(n=10)相比,银屑病患者中观察到 CD3+CD4+CXCR3+、CD3+CD4+CCR6+CCR4+CXCR3+(CXCR3+-Th17)和 CD3+CD4+CCR6+CCR4-CXCR3+(Th17.1)细胞群增加。IL-17 治疗性阻断降低了在应答性银屑病患者中的 CD3+CD4+CCR6+、CD3+CD4+CXCR3+、CD3+CD4+CCR6-CXCR3+(Th1)、CD3+CD4+CCR6+CCR4+(Th17)、CD3+CD4+CCR6+CCR4+CXCR3+(CXCR3+-Th17)和 CD3+CD4+CCR6+CCR4-CXCR3+(Th17.1)细胞群。此外,CD3+CD4-CCR6+、CD3+CD4-CXCR3+、CD3+CD4-CCR6+CCR4+(Tc17)和 CD3+CD4-CCR6-CXCR3+(Tc1)的百分比也受到抑制。还评估了用甲氨蝶呤(n=4)、阿普米司特(n=4)和抗 IL-23 生物治疗(n=4)治疗的患者中相同的细胞亚群的调节。在我们的研究中,首次探索了接受抗 IL-17 或抗 IL-17R 靶向生物治疗的银屑病患者外周血促炎 Th1、Th17 和额外的 CCR6+T 细胞亚群的水平和功能能力。我们的数据清楚地表明,早期抗 IL-17 介导的临床缓解伴随着 Th1、Th17、CXCR3+-Th17 和 Th17.1 细胞的显著减少。