Coppalini Giacomo, Duvigneaud Elie, Diosdado Alberto, Migliorino Ernesto, Schuind Sophie, Creteur Jacques, Taccone Fabio Silvio, Gouvêa Bogossian Elisa
Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles, Route de Lennik, Brussels, Belgium.
Department of Neurosurgery, Erasme Hospital, Université Libre de Bruxelles, Route de Lennik, Brussels, Belgium.
Front Neurol. 2022 Jul 19;13:963562. doi: 10.3389/fneur.2022.963562. eCollection 2022.
Tissue hypoxia and insufficient energy delivery is one of the mechanisms behind the occurrence of several complications in acute brain injured patients. Several interventions can improve cerebral oxygenation; however, the effects of inotropic agents remain poorly characterized.
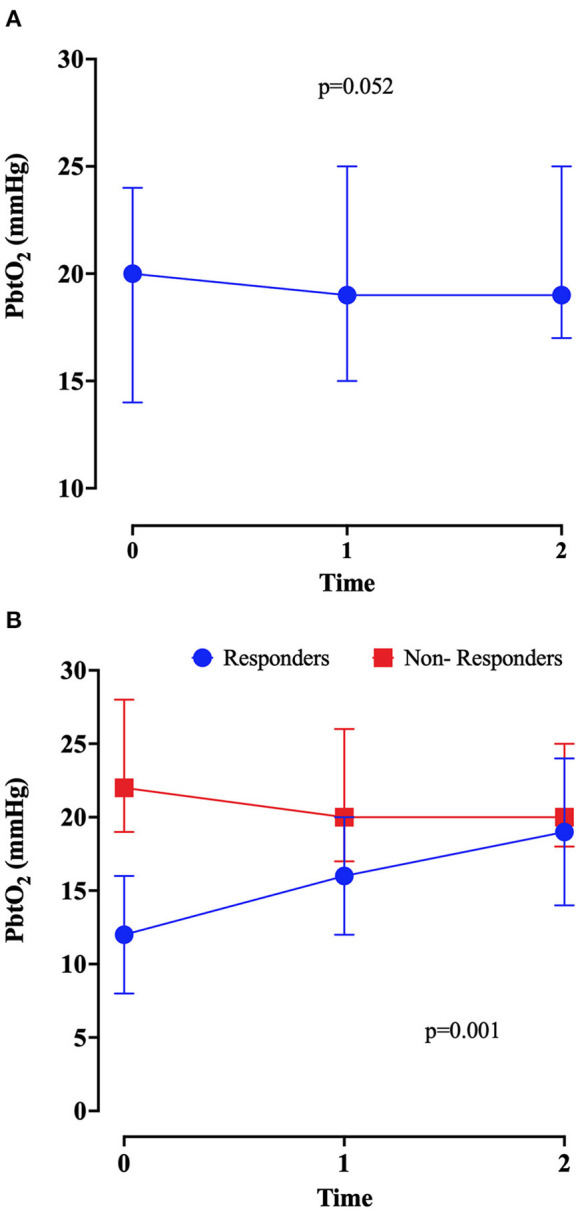
Retrospective analysis including patients suffering from acute brain injury and monitored with brain oxygen pressure (PbtO) catheter, in whom inotropic agents were administered according to the decision of the treating physician's decision; PbtO values were collected before, 1 and 2 h after the initiation of therapy from the patient data monitoring system. PbtO "responders" were patients with a relative increase in PbtO from baseline values of at least 20%.
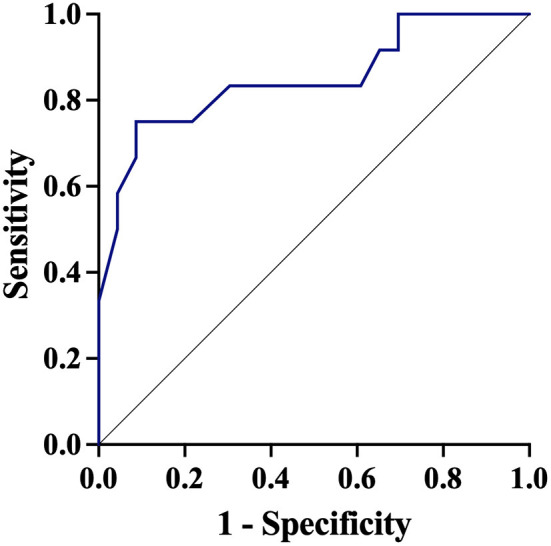
A total of 35 patients were included in this study. Most of them (31/35, 89%) suffered from non-traumatic subarachnoid hemorrhage (SAH). Compared with baseline values [20 (14-24) mmHg], PbtO did not significantly increase over time [19 (15-25) mmHg at 1 h and 19 (17-25) mmHg at 2 h, respectively; = 0.052]. A total of 12/35 (34%) patients were PbtO "responders," in particular if low PbtO was observed at baseline. A PbtO of 17 mmHg at baseline had a sensibility of 84% and a specificity of 91% to predict a PbtO responder. A significant direct correlation between changes in PbtO and cardiac output [r = 0.496 (95% CI 0.122 to 0.746), = 0.01; = 25] and a significant negative correlation between changes in PbtO and cerebral perfusion pressure [ = -0.389 (95% CI -0.681 to -0.010), = 0.05] were observed.
In this study, inotropic administration significantly increased brain oxygenation in one third of brain injured patients, especially when tissue hypoxia was present at baseline. Future studies should highlight the role of inotropic agents in the management of tissue hypoxia in this setting.
组织缺氧和能量供应不足是急性脑损伤患者发生多种并发症的机制之一。多种干预措施可改善脑氧合;然而,强心剂的作用仍未得到充分阐明。
回顾性分析纳入急性脑损伤且使用脑氧分压(PbtO)导管进行监测的患者,这些患者根据治疗医师的决定使用了强心剂;从患者数据监测系统收集治疗开始前、治疗开始后1小时和2小时的PbtO值。PbtO “反应者” 是指PbtO较基线值相对增加至少20% 的患者。
本研究共纳入35例患者。其中大多数(31/35,89%)患有非创伤性蛛网膜下腔出血(SAH)。与基线值[20(14 - 24)mmHg]相比,PbtO并未随时间显著增加[1小时时为19(15 - 25)mmHg,2小时时为19(17 - 25)mmHg;P = 0.052]。共有12/35(34%)例患者为PbtO “反应者”,特别是在基线时观察到低PbtO的患者。基线时PbtO为17 mmHg预测PbtO反应者的敏感性为84%,特异性为91%。观察到PbtO变化与心输出量之间存在显著的正相关[r = 0.496(95% CI 0.122至0.746),P = 0.01;n = 25],且PbtO变化与脑灌注压之间存在显著的负相关[P = -0.389(95% CI -0.681至 -0.010),P = 0.05]。
在本研究中,强心剂给药使三分之一的脑损伤患者脑氧合显著增加,尤其是在基线时存在组织缺氧的患者中。未来的研究应突出强心剂在这种情况下组织缺氧管理中的作用。