Department of Health Services Administration and Policy, Temple University, Philadelphia, PA, United States of America.
Department of Epidemiology, University of Alabama at Birmingham, Birmingham, AL, United States of America.
PLoS One. 2022 Aug 5;17(8):e0270675. doi: 10.1371/journal.pone.0270675. eCollection 2022.
Maintaining blood pressure (BP) control over time may contribute to lower risk for cardiovascular disease (CVD) among individuals who are taking antihypertensive medication.
The Jackson Heart Study (JHS) enrolled 5,306 African-American adults ≥21 years of age and was used to determine the proportion of African Americans that maintain persistent BP control, identify factors associated with persistent BP control, and determine the association of persistent BP control with CVD events. This analysis included 1,604 participants who were taking antihypertensive medication at Visit 1 and had BP data at Visits 1 (2000-2004), 2 (2005-2008), and 3 (2009-2013). Persistent BP control was defined as systolic BP <140 mm Hg and diastolic BP <90 mm Hg at all three visits. CVD events were assessed from Visit 3 through December 31, 2016. Hazard ratios (HR) for the association of persistent BP control with CVD outcomes were adjusted for age, sex, systolic BP, smoking, diabetes, and total and high-density lipoprotein cholesterol at Visit 3.
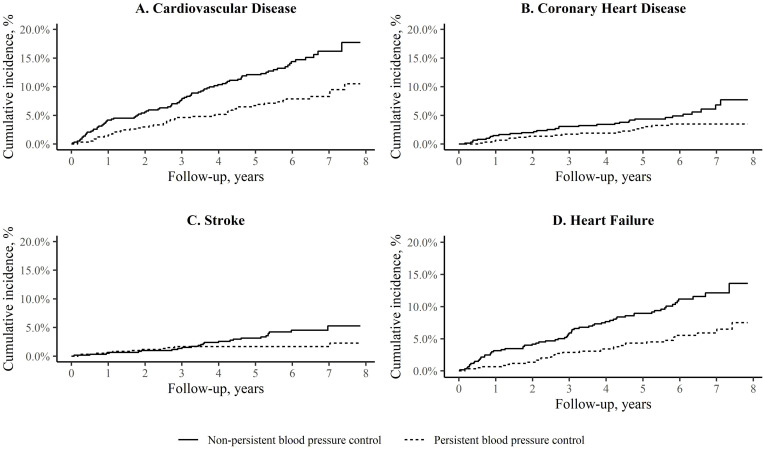
At Visit 1, 1,226 of 1,604 participants (76.4%) with hypertension had controlled BP. Overall, 48.9% of participants taking antihypertensive medication at Visit 1 had persistent BP control. After multivariable adjustment for demographic, socioeconomic, clinical, behavioral, and psychosocial factors, and access-to-care, participants were more likely to have persistent BP control if they were <65 years of age, women, had family income ≥$25,000 at each visit, and visited a health professional in the year prior to each visit. The multivariable adjusted HR (95% confidence interval) comparing participants with versus without persistent BP control was 0.71 (0.46-1.10) for CVD, 0.68 (0.34-1.34) for coronary heart disease, 0.65 (0.27-1.52) for stroke, and 0.55 (0.33-0.90) for heart failure.
Less than half of JHS participants taking antihypertensive medication had persistent BP control, putting them at increased risk for heart failure.
对于正在服用抗高血压药物的个体,随着时间的推移维持血压控制可能有助于降低心血管疾病(CVD)的风险。
杰克逊心脏研究(JHS)纳入了 5306 名年龄≥21 岁的非裔美国成年人,用于确定维持持续性血压控制的非裔美国人比例,确定与持续性血压控制相关的因素,并确定持续性血压控制与 CVD 事件的相关性。这项分析包括 1604 名在第一次就诊时服用抗高血压药物且在第一次就诊(2000-2004 年)、第二次就诊(2005-2008 年)和第三次就诊(2009-2013 年)时具有血压数据的参与者。持续性血压控制定义为三次就诊时的收缩压<140mmHg 和舒张压<90mmHg。从第三次就诊开始评估 CVD 事件,直至 2016 年 12 月 31 日。调整第三次就诊时的年龄、性别、收缩压、吸烟、糖尿病以及总胆固醇和高密度脂蛋白胆固醇后,持续性血压控制与 CVD 结局的关联的风险比(HR)。
在第一次就诊时,1604 名高血压患者中有 1226 名(76.4%)血压得到控制。总体而言,在第一次就诊时服用抗高血压药物的参与者中有 48.9%具有持续性血压控制。在调整人口统计学、社会经济、临床、行为和社会心理因素以及医疗保健可及性后,与年龄<65 岁、女性、每次就诊时家庭收入≥$25000 以及在每次就诊前一年就诊过卫生专业人员的参与者相比,他们更有可能具有持续性血压控制。与没有持续性血压控制的参与者相比,多变量调整后的 HR(95%置信区间)为 CVD(0.71[0.46-1.10])、冠心病(0.68[0.34-1.34])、中风(0.65[0.27-1.52])和心力衰竭(0.55[0.33-0.90])。
JHS 中服用抗高血压药物的参与者中不到一半具有持续性血压控制,这使他们面临心力衰竭的风险增加。