University Hospital Arnau de Vilanova, Lleida, Spain.
IRBLLeida (Institut de Recerca Biomèdica de Lleida), Lleida, Spain.
J Interv Cardiol. 2022 Jul 21;2022:7932114. doi: 10.1155/2022/7932114. eCollection 2022.
Distal radial access for coronary procedures decreases hemostasis time, prevents radial occlusion, and improves patient comfort compared to conventional transradial access. Initially described for left distal radial access (lDRA), the right distal radial access (rDRA) is feasible. However, there are no comparative studies to date. This study aimed to evaluate the impact of the access site on vascular access and procedural performance.
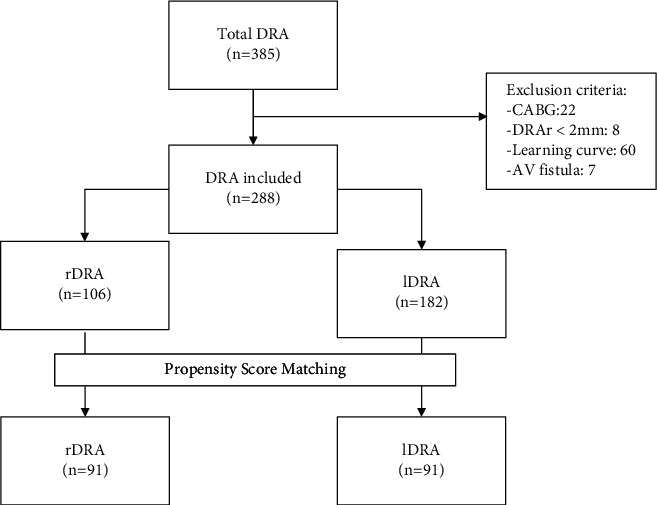
From August 2020 to October 2021, coronary procedures performed through distal radial access were prospectively recorded. After propensity score matching, the rDRA and lDRA were compared. The primary endpoint was the proportion of approach success. The secondary endpoints included access time, coronary procedural success, radial spasm, exposition to ionizing radiation, patient comfort, and vascular access-related complications.
From a total of 385 procedures in 382 patients, after a propensity score matching, 182 procedures were compared between the rDRA and lDRA. There were no differences in the baseline characteristics between the groups. Compared to the lDRA, the rDRA presented similar approach success (96.7% vs. 96.7%, =1.0), less access time (39 (25-60) sec vs. 50 (29-90) sec, =0.018), comparable coronary procedural success after sheath placement (100% vs. 100%, =1.000), and not statistically significant radial spasm (2.19% vs. 6.59%, =0.148). No differences in dose-area product (32 (20-56.2) Gy.m2 vs. 32.3 (19.4-46.3) Gy.m2; =0.472) and fluoroscopy time (4.4 (2.5-9.1) min vs. 4.3 (2.4-7.5) min, =0.251) were detected between the groups. No vascular access-related complications were observed in any group.
The rDRA, compared to the lDRA, had the same proportion of approach success and procedural performance, with a slight reduction in access time for patients undergoing coronary procedures.
与传统经桡动脉入路相比,经远端桡动脉入路(DRA)进行冠状动脉介入治疗可减少止血时间、预防桡动脉闭塞并提高患者舒适度。虽然最初是为左远端桡动脉入路(lDRA)而描述的,但右远端桡动脉入路(rDRA)也是可行的。然而,目前尚无相关的比较研究。本研究旨在评估入路部位对血管入路和程序性能的影响。
2020 年 8 月至 2021 年 10 月,前瞻性地记录了通过远端桡动脉入路进行的冠状动脉介入治疗。在进行倾向评分匹配后,比较了 rDRA 和 lDRA。主要终点是入路成功率。次要终点包括入路时间、冠状动脉介入治疗成功率、桡动脉痉挛、放射暴露、患者舒适度和血管入路相关并发症。
在总共 382 名患者的 385 例手术中,在进行倾向评分匹配后,对 rDRA 和 lDRA 之间的 182 例手术进行了比较。两组患者的基线特征无差异。与 lDRA 相比,rDRA 的入路成功率相似(96.7%比 96.7%,=1.0),入路时间更短(39(25-60)s 比 50(29-90)s,=0.018),在鞘管置入后冠状动脉介入治疗成功率相当(100%比 100%,=1.000),桡动脉痉挛的发生率也无统计学差异(2.19%比 6.59%,=0.148)。两组间剂量面积乘积(32(20-56.2)Gy·m2 比 32.3(19.4-46.3)Gy·m2;=0.472)和透视时间(4.4(2.5-9.1)min 比 4.3(2.4-7.5)min;=0.251)无差异。两组均未发生血管入路相关并发症。
与 lDRA 相比,rDRA 的入路成功率和程序性能相当,而接受冠状动脉介入治疗的患者的入路时间略有缩短。