Guru Satyabrata, Singh Neha, Sahoo Sangeeta, Hansda Upendra, Mohanty Chittaranjan
Department of Trauma and Emergency, AIIMS, Bhubaneswar, Odisha, India.
Department of Anaesthesiology, AIIMS, Bhubaneswar, Odisha, India.
Turk J Emerg Med. 2022 Jul 1;22(3):149-155. doi: 10.4103/2452-2473.348436. eCollection 2022 Jul-Sep.
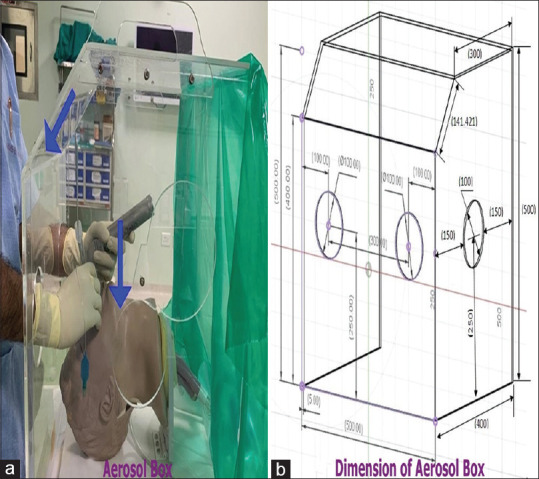
Coronavirus disease 2019 (COVID-19) virus usually spreads through aerosol and close contact. Frontline health-care workers handle aerosol-generating procedures like endotracheal intubation. To reduce this risk, COVID-19 barrier box came into the picture. However, the COVID-19 barrier box may compromise easy and successful intubation, and their limitation must be studied.
The objective of this study was to assess the time to successful intubation with or without the COVID-19 barrier box using the Macintosh laryngoscope and King Vision video laryngoscope (KVVL). We also assessed the first-pass success rate, ease of intubation, Cormack-Lehane (CL) grade, and requirement of external laryngeal manipulation.
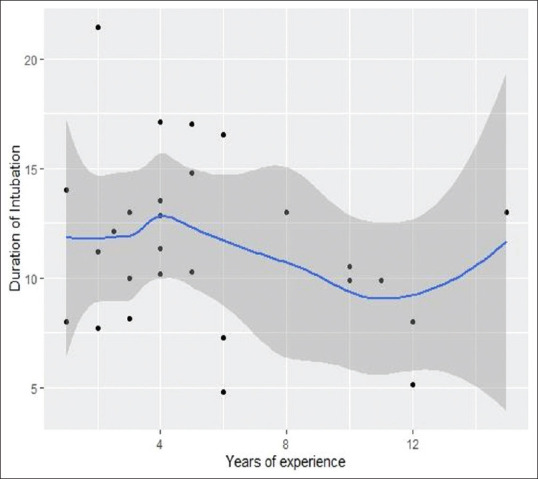
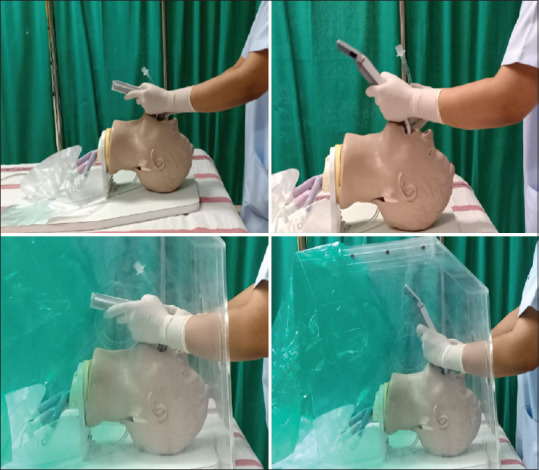
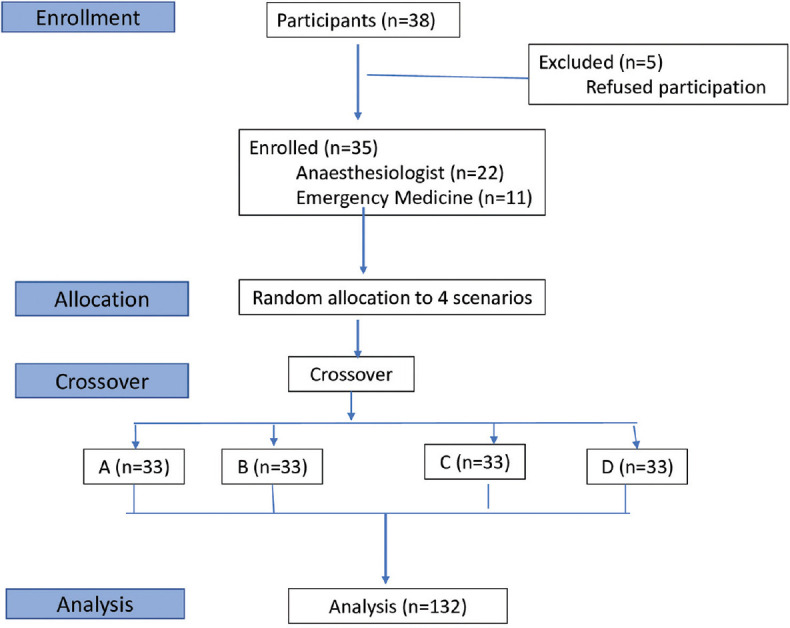
We conducted this manikin-based randomized crossover study to assess the time to successful intubation by anesthesiologists (22) and emergency physicians (11) having 1 year or more experience with or without COVID-19 barrier box by using the Macintosh laryngoscope and KVVL. Our study randomized the sequence of the four different intubation scenarios.
The comparison of mean duration of intubation between KVVL (13.21 ± 4.05 s) and Macintosh laryngoscope (12.89 ± 4.28 s) with COVID-19 barrier box was not statistically significant (95% confidence interval: 1.21-0.97). The ease of intubation, number of attempts, and requirement of external laryngeal manipulation were not statistically significant. Intubations were statistically significant more difficult with barrier box in view of higher CL grade.
Time to intubation was longer with COVID-19 barrier box using KVVL as compared to Macintosh laryngoscope which was statistically not significant.
2019冠状病毒病(COVID-19)病毒通常通过气溶胶和密切接触传播。一线医护人员会进行如气管插管等产生气溶胶的操作。为降低这种风险,COVID-19防护箱应运而生。然而,COVID-19防护箱可能会影响气管插管的顺利进行,其局限性必须加以研究。
本研究的目的是评估使用麦金托什喉镜和可视喉镜(KVVL)在有或没有COVID-19防护箱的情况下成功插管的时间。我们还评估了首次通过成功率、插管的难易程度、科马克-莱汉内(CL)分级以及外部喉操作的需求。
我们进行了这项基于人体模型的随机交叉研究,以评估有1年或以上经验的麻醉医生(22名)和急诊医生(11名)在使用麦金托什喉镜和KVVL且有或没有COVID-19防护箱的情况下成功插管的时间。我们的研究将四种不同插管场景的顺序进行了随机化。
使用COVID-19防护箱时,KVVL(13.21±4.05秒)和麦金托什喉镜(12.89±4.28秒)之间的平均插管持续时间比较无统计学意义(95%置信区间:1.21 - 0.97)。插管的难易程度、尝试次数和外部喉操作的需求无统计学意义。鉴于CL分级较高,使用防护箱时插管在统计学上更困难。
与麦金托什喉镜相比,使用KVVL时COVID-19防护箱的插管时间更长,但在统计学上无显著差异。