Department of Oncology, Xiangya Hospital, Central South University, Changsha, China.
Department of Pharmacy, Xiangya Hospital, Central South University, Changsha, China.
Front Public Health. 2022 Jul 22;10:947375. doi: 10.3389/fpubh.2022.947375. eCollection 2022.
The treatment paradigm of unresectable malignant pleural mesothelioma (MPM) has changed in recent years. Checkmate 743 demonstrate that nivolumab plus ipilimumab showed good clinical benefits compared with chemotherapy in the treatment of MPM. The study is aim to evaluate the cost-effectiveness of Nivolumab plus ipilimumab vs. platinum plus chemotherapy for the first-line treatment of unresectable MPM.
A Markov model was developed to compare the cost and quality-adjusted life-year (QALY) of nivolumab plus ipilimumab and chemotherapy over a 10-year time horizon. Clinical efficacy and safety data were extracted from the CheckMate 743 trials. Health state utilities were obtained from published literature. Costs were collected from an US payer perspective. One-way and probabilistic sensitivity analyses were conducted to explore the impact of uncertainties on the cost-effectiveness's results.
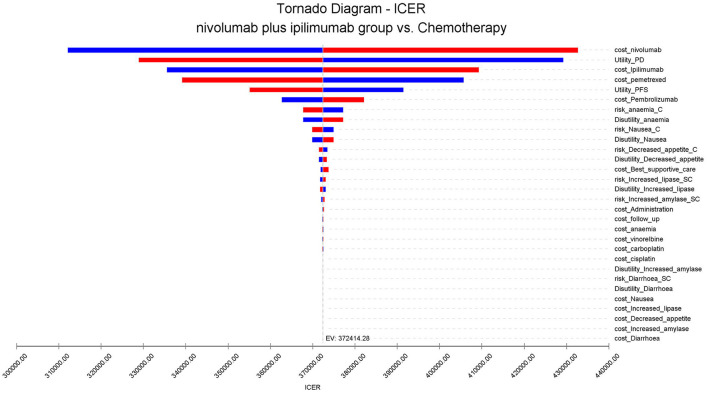
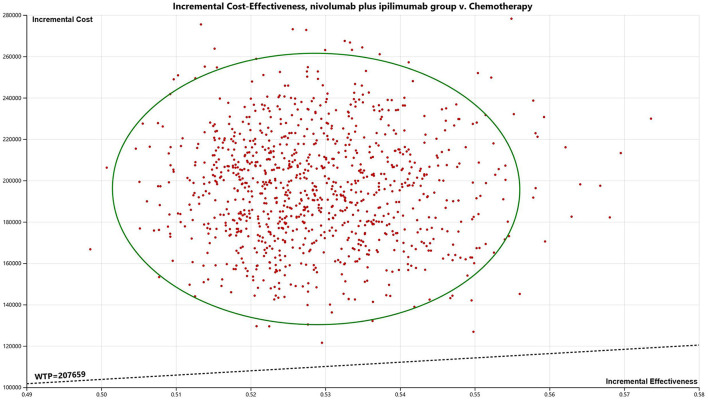
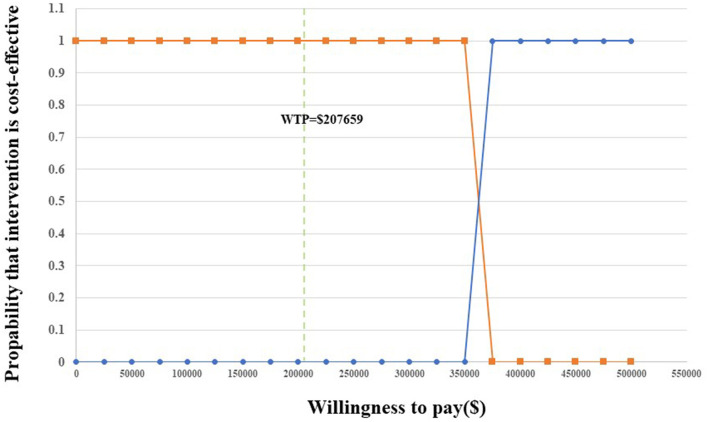
In the base case analysis, the incremental healthcare costs and QALYs for Nivolumab plus Ipilimumab vs. chemotherapy are $196,604.22 and 0.53, respectively, resulting an incremental cost-effectiveness ratio (ICER) of $372,414.28/QALYs for the model cohort of patients with locally advanced or metastatic MPM. However, Probabilistic sensitivity analysis showed that there was no probability that Nivolumab plus ipilimumab was cost-effective within the fluctuation range of other model parameters in first-line in unresectable MPM. The results of one-way sensitivity analysis showed that the cost of Nivolumab was the most sensitive parameter.
The ICER of Nivolumab plus ipilimumab is above the theoretical willingness-to-pay threshold in the U.S, which suggests that first-line nivolumab plus ipilimumab for unresectable MPM may be not a cost-effective choice.
近年来,不可切除的恶性胸膜间皮瘤(MPM)的治疗模式发生了变化。Checkmate 743 表明,纳武单抗联合伊匹单抗在治疗 MPM 方面比化疗具有更好的临床获益。本研究旨在评估纳武单抗联合伊匹单抗与铂类化疗联合化疗作为不可切除 MPM 一线治疗的成本效益。
建立了一个 Markov 模型,以比较纳武单抗联合伊匹单抗与化疗在 10 年时间内的成本和质量调整生命年(QALY)。从 CheckMate 743 试验中提取临床疗效和安全性数据。健康状态效用值取自已发表的文献。从美国支付者的角度收集成本。进行了单因素和概率敏感性分析,以探讨不确定性对成本效益结果的影响。
在基线分析中,纳武单抗联合伊匹单抗与化疗相比,医疗保健增量成本和 QALY 分别为 196604.22 美元和 0.53,导致模型队列中局部晚期或转移性 MPM 患者的增量成本效益比(ICER)为 372414.28 美元/QALY。然而,概率敏感性分析表明,在不可切除 MPM 的一线治疗中,纳武单抗联合伊匹单抗没有达到其他模型参数波动范围内的成本效益的概率。单因素敏感性分析的结果表明,纳武单抗的成本是最敏感的参数。
纳武单抗联合伊匹单抗的 ICER 高于美国的理论意愿支付阈值,这表明纳武单抗联合伊匹单抗作为不可切除 MPM 的一线治疗可能不是一种具有成本效益的选择。