Carrera de Medicina Humana, Facultad de Ciencias de la Salud, Universidad Científica del Sur, Lima, Peru.
Grupo Estudiantil de Investigación en Salud Mental (GISAM), Sociedad Científica de Estudiantes de Medicina de la Universidad de San Martin de Porres, Universidad de San Martín de Porres, Lima, Peru.
Dis Markers. 2022 Aug 3;2022:2497202. doi: 10.1155/2022/2497202. eCollection 2022.
The prognostic value of the neutrophil-lymphocyte ratio (NLR) and platelet-lymphocyte ratio (PLR) in patients with COVID-19 is rarely described in older adults. We aimed to estimate the prognostic value of NLR and PLR, determining the mortality of adults over 60 years of age hospitalized for COVID-19 in three hospitals in Peru from March to May 2020.
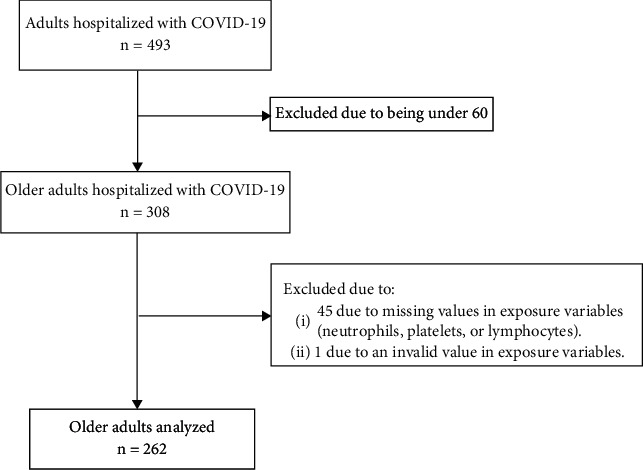
We performed a secondary analysis of data from a retrospective cohort carried out in Lambayeque, Peru, from March 18 to May 13, 2020. Older adults hospitalized for COVID-19 were included. The outcome variable was in-hospital mortality by all causes, while the exposure variable was the NLR and PLR (categorized in tertiles and numerically, performing a logarithmic transformation). We included sociodemographic variables, comorbidities, vital functions, laboratory markers, and treatment received during hospital stay. We evaluated the association between NLR and PLR using the hazard ratio (HR) in a Cox regression model. We estimated HR with their respective 95% confidence intervals (95% CI). We estimated cumulative/dynamic time-dependent ROC curves and reported area under the curve ROC (AUC-ROC) for 15-, 30-, and 60-day mortality with their respective simultaneous confidence intervals (confidence bands (CB)). Also, we estimated an optimal cut-off point based on the maximally selected rank statistics.
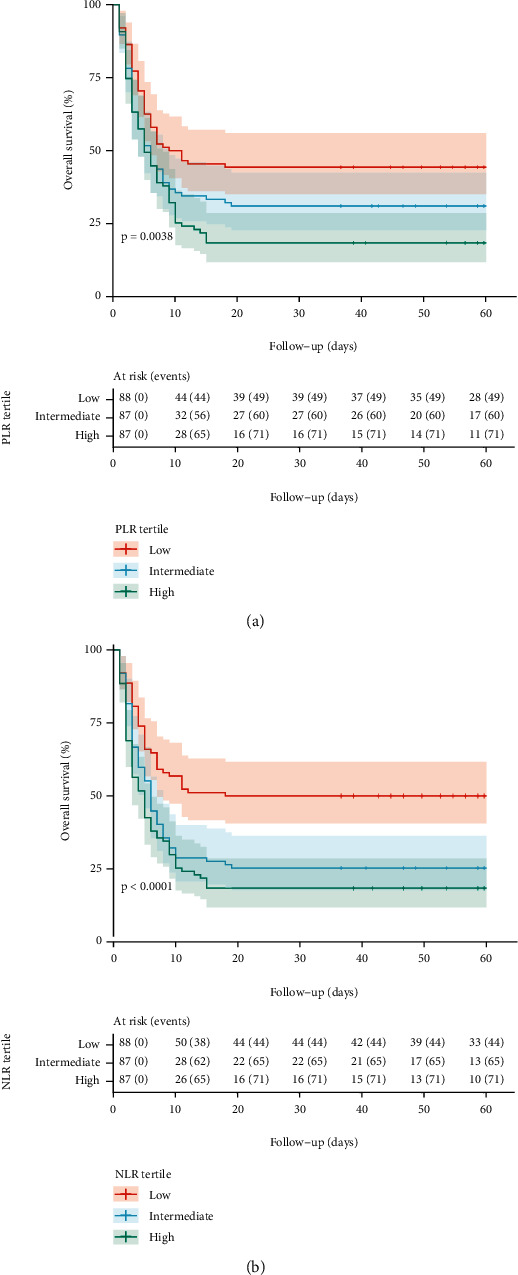
A total of 262 hospitalized older adults were analyzed, 71.8% ( = 188) of whom were male with a median age of 70 years (interquartile range: 65-78). The mean NLR and PLR were 16.8 (95% CI: 14.9-18.7; SD: 15.5) and 50.3 (95% CI: 44.6-55.9; SD: 46.3), respectively. The mortality rate was 68.7% (95% CI: 62.7-74.3). The adjusted Cox regression analysis showed that the high NLR (adjusted HR (aHR) = 2.12; 95% CI: 1.43-3.14) and PLR (aHR = 1.90; 95% CI: 1.30-2.79) tertiles were associated with a higher risk of mortality. The maximum AUC-ROC values at 60 days of follow-up for NLR and PLR were 0.713 (95%CB: 0.627-0.800) and 0.697 (95%CB: 0.583-0.754), respectively.
The NLR and PLR are predictors of higher risk of mortality, and these results suggest that both could be reliable and practical markers for the identification of older adults at high risk of mortality by COVID-19. NLR and PLR have prognostic value, with an AUC greater than 0.5; however, by themselves, they are weak prognostic markers. It is important to carry out future studies incorporating these two markers into preexisting models or designing new ones considering them.
中性粒细胞与淋巴细胞比值(NLR)和血小板与淋巴细胞比值(PLR)在 COVID-19 患者中的预后价值在老年人中很少被描述。我们旨在评估 NLR 和 PLR 的预后价值,确定 2020 年 3 月至 5 月期间秘鲁 3 家医院住院的 60 岁以上成年人 COVID-19 的死亡率。
我们对秘鲁 Lambayeque 进行的回顾性队列研究的数据进行了二次分析,时间为 2020 年 3 月 18 日至 5 月 13 日。包括因 COVID-19 住院的老年人。因变量为全因住院死亡率,而暴露变量为 NLR 和 PLR(分为三分位和数值,对数转换)。我们纳入了社会人口统计学变量、合并症、生命体征、实验室标志物以及住院期间接受的治疗。我们使用 Cox 回归模型中的风险比(HR)评估 NLR 和 PLR 之间的相关性。我们用各自的 95%置信区间(95%CI)估计 HR。我们估计了 15、30 和 60 天死亡率的累积/动态时间依赖性 ROC 曲线,并报告了曲线下面积 ROC(AUC-ROC)及其各自的同时置信区间(置信带(CB))。此外,我们还根据最大选择秩统计量确定了最佳截断点。
共分析了 262 名住院的老年人,其中 71.8%(=188)为男性,中位年龄为 70 岁(四分位间距:65-78)。平均 NLR 和 PLR 分别为 16.8(95%CI:14.9-18.7;SD:15.5)和 50.3(95%CI:44.6-55.9;SD:46.3)。死亡率为 68.7%(95%CI:62.7-74.3)。调整后的 Cox 回归分析表明,高 NLR(调整后 HR[aHR] = 2.12;95%CI:1.43-3.14)和 PLR(aHR = 1.90;95%CI:1.30-2.79)三分位与更高的死亡率风险相关。NLR 和 PLR 在 60 天随访时的最大 AUC-ROC 值分别为 0.713(95%CB:0.627-0.800)和 0.697(95%CB:0.583-0.754)。
NLR 和 PLR 是死亡率风险较高的预测因子,这些结果表明,这两者都可能是识别 COVID-19 高危死亡率的可靠且实用的标志物。NLR 和 PLR 具有预后价值,AUC 大于 0.5;然而,它们本身是弱的预后标志物。重要的是要进行未来的研究,将这两个标志物纳入现有的模型或设计新的模型来考虑它们。