Li Na, Liu Penghui, Guo Jiwu, Wang Jizhen, Han Xinling, Mao Jie
Lanzhou University Second Clinical Medical College, Lanzhou, China.
Lanzhou University Second Hospital, Lanzhou, China.
Front Med (Lausanne). 2025 Aug 5;12:1605819. doi: 10.3389/fmed.2025.1605819. eCollection 2025.
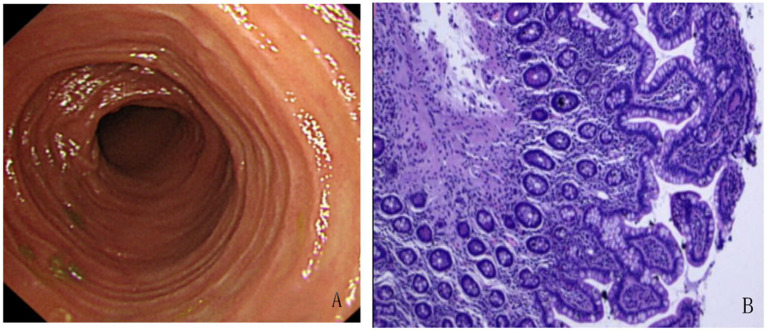
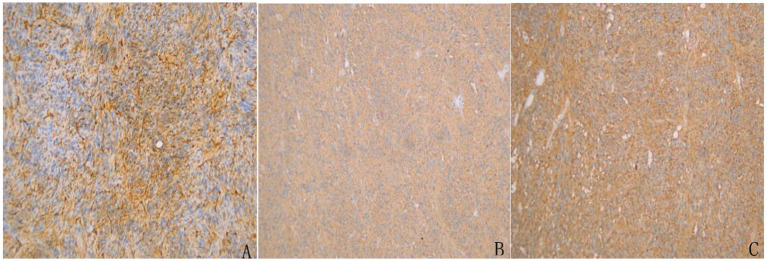
Gastrointestinal stromal tumor (GIST) with secondary thrombocytosis is a rare clinical case, exhibiting specificity in clinical diagnosis and treatment. We report a case of GIST with secondary thrombocythemia to raise clinicians' attention to this disease. On October 11, 2024, a 58-year-old male patient was admitted to the hospital due to "intermittent right lower abdominal pain with increased bowel movements for more than 1 month." The patient had no prior history of tumors, chronic inflammatory diseases, hematologic disorders or family history of genetic disorders. MRI-enhanced scans of the small intestine highly indicated a lymphoma of intestinal origin. Small bowel endoscopy and pathological biopsy revealed mild chronic inflammation of the intestinal mucosa, with intact villous architecture, no plasmacytosis, granulomas, or vasculitis, and no indication of GIST. Laboratory tests showed platelet count of 909 × 10/L, white blood cell count of 11.86 × 10/L, neutrophil ratio of 75.10%, lymphocyte ratio of 15.30% and hemoglobin 101 g/L. Bone marrow biopsy microscopically showed a normal number of megakaryocytes without abnormal aggregation and no myelofibrosis, suggesting there was no obvious hematologic malignancy and the thrombocytosis may have been secondary. The patient underwent partial resection of the small intestine and resection of mesenteric lesions on October 18, 2024. The intraoperative frozen section suggested a stromal tumor. The postoperative pathological biopsy suggested a GIST and genetic testing showed a mutation in the c-KIT gene (Exon 13). Postoperatively, the patient was treated with oral imatinib mesylate (400 mg/d) as adjunctive therapy. Three months after surgery, imaging showed no recurrence, platelet decreased and returned to normal levels.
胃肠道间质瘤(GIST)伴继发性血小板增多症是一种罕见的临床病例,在临床诊断和治疗方面具有特殊性。我们报告一例GIST伴继发性血小板增多症病例,以提高临床医生对该病的关注。2024年10月11日,一名58岁男性患者因“间断右下腹痛伴排便次数增多1个多月”入院。患者既往无肿瘤、慢性炎症性疾病、血液系统疾病史或遗传性疾病家族史。小肠MRI增强扫描高度提示为肠道原发性淋巴瘤。小肠内镜及病理活检显示肠黏膜轻度慢性炎症,绒毛结构完整,无浆细胞增多、肉芽肿或血管炎,未提示GIST。实验室检查显示血小板计数909×10⁹/L,白细胞计数11.86×10⁹/L,中性粒细胞比例75.10%,淋巴细胞比例15.30%,血红蛋白101g/L。骨髓活检显微镜下显示巨核细胞数量正常,无异常聚集,无骨髓纤维化,提示无明显血液系统恶性肿瘤,血小板增多可能为继发性。2024年10月18日,患者接受小肠部分切除术及肠系膜病变切除术。术中冰冻切片提示为间质瘤。术后病理活检提示为GIST,基因检测显示c-KIT基因(外显子13)突变。术后,患者接受口服甲磺酸伊马替尼(400mg/d)辅助治疗。术后3个月,影像学检查显示无复发,血小板下降并恢复至正常水平。