Awadelkarim Abdalaziz, Yassin Ahmed S, Ali Mohammed, Dayco John, Saad Eltaib, Idris Isra, Alhusain Rashid, Sebastian Joseph, Afonso Luis
Department of Internal Medicine, Wayne State University/Detroit Medical Center, Detroit, MI, USA.
Department of Cardiology, Wayne State University/Detroit Medical Center, Detroit, MI, USA.
J Med Cases. 2022 Jul;13(7):341-348. doi: 10.14740/jmc3946. Epub 2022 Jul 20.
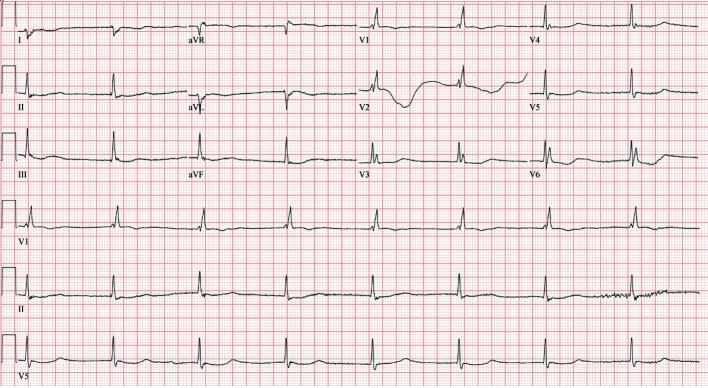
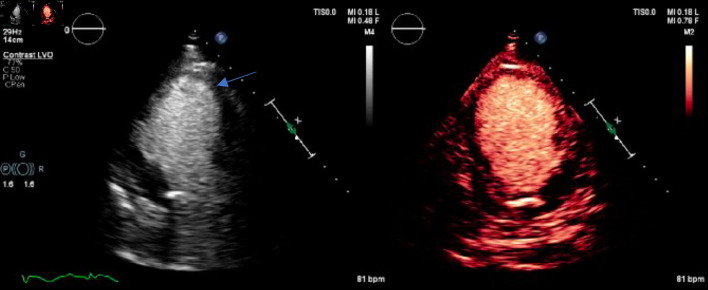
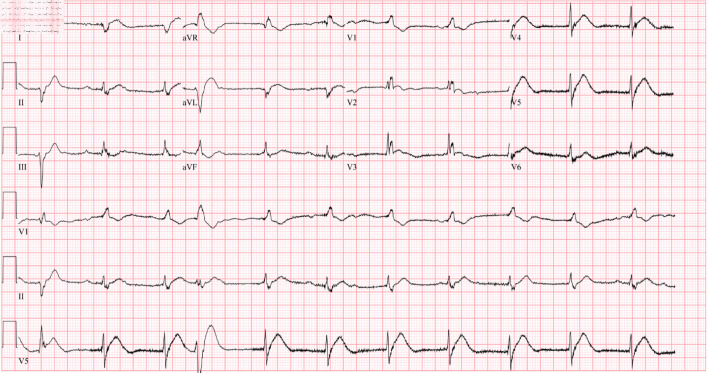
QT prolongation is present in 26-52% of cases of Takotsubo cardiomyopathy (TCM). It has been postulated to result from reduced cardiac repolarization reserve and reflects the transient myocardial insult observed in TCM. Bradycardia-induced QT interval prolongation is amplified by the occurrence of TCM, a combination that potentially carries a significant risk for torsade de pointes (TdP). We present a unique case of an 80-year-old female with TCM-related cardiac arrest. The patient had acquired long QT syndrome in which TCM myocardial insult led to the precipitation of a third-degree atrioventricular (AV) block and subsequent bradycardia-induced TdP. Due to the lack of robust literature, there is no clear guideline in the management of third-degree AV block in the setting of TCM. In our case, because of recurrent ventricular tachycardia (VT) and ventricular fibrillation (VF) arrest, we opted for temporary pacing at a high ventricular rate, followed by a biventricular implantable cardioverter-defibrillator (BiV/ICD). Follow-up 3 months later revealed improvement of left ventricular (LV) dysfunction and resolution of QT prolongation. However, the noticed AV conduction defects persisted. In the available literature, we identified five reported cases that bear similarity with our patient's presentation. The identified cases were middle-aged to elderly females with no significant cardiac history, who exhibited a similar triad of TCM associated with high-grade AV block, acquired long QT syndrome, and a rapid progression of bradycardia-induced TdP, resulting in a near cardiac arrest within the first 24 - 48 h of admission. It is crucial to monitor corrected QT (QTc), correct electrolyte abnormalities, and minimize QT-prolonging medications in patients with TCM. The recognition of AV conduction defects in patients with TCM is critical, especially if it is associated with significant QT prolongation. Such situations are underrecognized, and are potentially fatal, necessitating close monitoring and timely intervention.
在26%-52%的应激性心肌病(TCM)病例中存在QT间期延长。据推测,这是由于心脏复极储备减少所致,反映了在TCM中观察到的短暂性心肌损伤。TCM的发生会放大心动过缓引起的QT间期延长,这种组合可能会带来显著的尖端扭转型室速(TdP)风险。我们报告了一例80岁女性因TCM导致心脏骤停的独特病例。该患者患有获得性长QT综合征,其中TCM心肌损伤导致三度房室(AV)传导阻滞的发生以及随后心动过缓诱发的TdP。由于缺乏有力的文献资料,在TCM背景下三度AV传导阻滞的管理尚无明确指南。在我们的病例中,由于反复出现室性心动过速(VT)和心室颤动(VF)骤停,我们选择了高心室率临时起搏,随后植入双心室植入式心脏复律除颤器(BiV/ICD)。3个月后的随访显示左心室(LV)功能障碍有所改善,QT间期延长得到缓解。然而,所发现的AV传导缺陷仍然存在。在现有文献中,我们找到了5例与我们患者表现相似的报告病例。所发现的病例为中年至老年女性,无显著心脏病史,并表现出类似的三联征,即TCM合并高度AV传导阻滞、获得性长QT综合征以及心动过缓诱发的TdP快速进展,导致入院后最初24 - 48小时内接近心脏骤停。对于TCM患者,监测校正QT(QTc)、纠正电解质异常以及尽量减少延长QT的药物至关重要。认识到TCM患者的AV传导缺陷至关重要,尤其是当它与显著的QT间期延长相关时。这种情况未得到充分认识,且可能致命,需要密切监测和及时干预。