Department of Pediatrics, Severance Children's Hospital, Institute of Allergy, Brain Korea 21 PLUS Project for Medical Science, Yonsei University College of Medicine, 50-1, Yonsei-ro, Seodaemun-gu, Seoul, 03722, Republic of Korea.
Department of Pediatrics, Kyung Hee University College of Medicine, Seoul, Republic of Korea.
Sci Rep. 2022 Aug 11;12(1):13666. doi: 10.1038/s41598-022-18038-6.
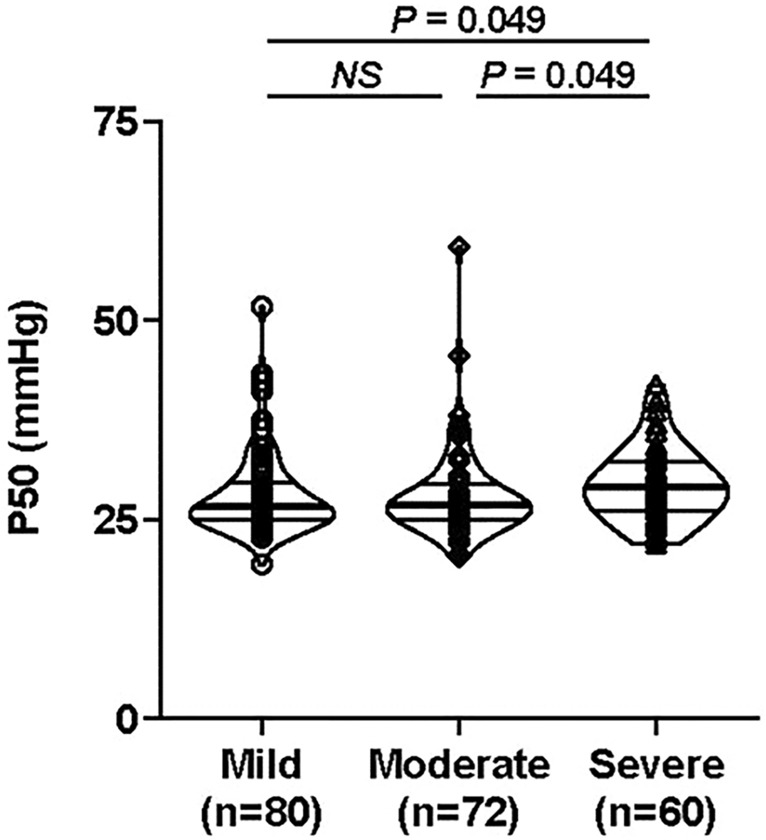
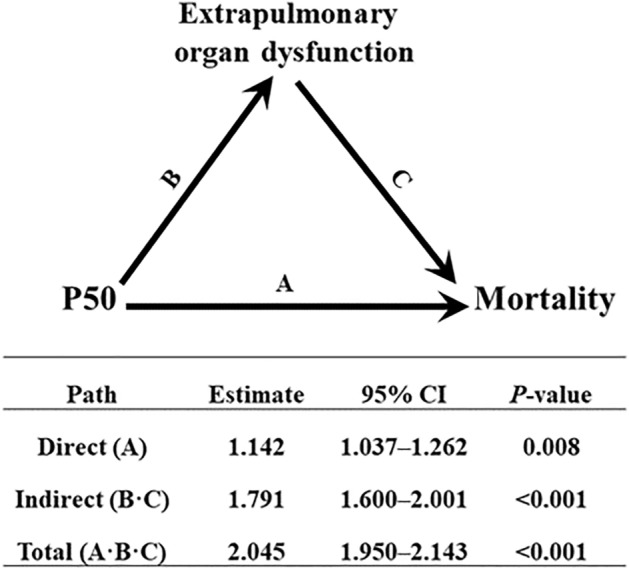
Hypoxemia and multiple organ dysfunction are significant contributors to mortality in patients with pediatric acute respiratory distress syndrome (PARDS). P50, the oxygen tension at which hemoglobin is 50% saturated, is a measure of hemoglobin-oxygen affinity, and its alteration might have implications for tissue hypoxia and organ dysfunction. The purpose of this single-center, retrospective study was to evaluate P50 levels in PARDS and to determine the association between P50 and clinical outcomes. The study included 212 children diagnosed with PARDS according to the Pediatric Acute Lung Injury Consensus Conference definition who required invasive mechanical ventilation and had arterial blood gas results of hemoglobin oxygen saturation < 97% at the time of diagnosis. P50 levels were calculated using Doyle's method, and organ dysfunction was assessed using the Pediatric Logistic Organ Dysfunction-2 score. Most patients exhibited more than one dysfunctional extrapulmonary organ at PARDS onset. P50 increased with increasing PARDS severity (mild (26.6 [24.9-29.6]), moderate (26.8 [25.0-29.5]), and severe PARDS (29.1 [26.1-32.4] mmHg; P = 0.025). Moreover, P50 demonstrated a significant positive association with extrapulmonary organ dysfunction score (β = 0.158, P = 0.007) and risk of mortality (adjusted hazard ratio, 1.056; 95% confidence interval, 1.015-1.098; P = 0.007), irrespective of initial PARDS severity. The relationship between P50 and mortality was largely mediated by extrapulmonary organ dysfunction. A high P50 value at the time of PARDS diagnosis may be associated with mortality via dysfunctional extrapulmonary organs. Future studies should consider P50 as a potential candidate index for risk stratification of PARDS patients.
低氧血症和多器官功能障碍是小儿急性呼吸窘迫综合征(PARDS)患者死亡的重要原因。P50 是血红蛋白饱和度为 50%时的氧分压,是血红蛋白-氧亲和力的度量,其改变可能对组织缺氧和器官功能障碍有影响。本单中心回顾性研究的目的是评估 PARDS 患者的 P50 水平,并确定 P50 与临床结局之间的关系。该研究纳入了 212 名根据小儿急性肺损伤共识会议定义诊断为 PARDS 的儿童,这些儿童需要有创机械通气,并且在诊断时动脉血气血红蛋白氧饱和度 < 97%。P50 水平使用 Doyle 法计算,器官功能障碍使用小儿逻辑器官功能障碍-2 评分评估。大多数患者在 PARDS 发病时表现出超过一个肺外器官功能障碍。随着 PARDS 严重程度的增加,P50 增加(轻度(26.6 [24.9-29.6])、中度(26.8 [25.0-29.5])和重度 PARDS(29.1 [26.1-32.4] mmHg;P=0.025)。此外,P50 与肺外器官功能障碍评分呈显著正相关(β=0.158,P=0.007)和死亡率(调整后的危险比,1.056;95%置信区间,1.015-1.098;P=0.007),与初始 PARDS 严重程度无关。P50 与死亡率之间的关系主要由肺外器官功能障碍介导。PARDS 诊断时 P50 值较高可能通过肺外器官功能障碍与死亡率相关。未来的研究应考虑将 P50 作为 PARDS 患者风险分层的潜在候选指标。