Spadaro Savino, Park Mirae, Turrini Cecilia, Tunstall Tanushree, Thwaites Ryan, Mauri Tommaso, Ragazzi Riccardo, Ruggeri Paolo, Hansel Trevor T, Caramori Gaetano, Volta Carlo Alberto
1Department of Morphology, Surgery and Experimental Medicine, Intensive Care Section, University of Ferrara, 44121 Ferrara, Italy.
2Faculty of Medicine, National Heart and Lung Institute, Imperial College London, London, UK.
J Inflamm (Lond). 2019 Jan 15;16:1. doi: 10.1186/s12950-018-0202-y. eCollection 2019.
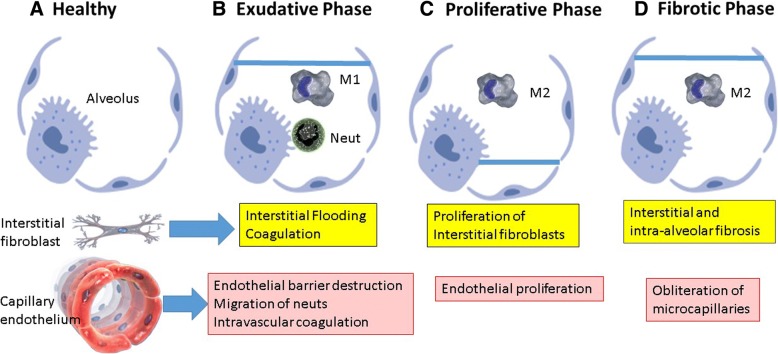
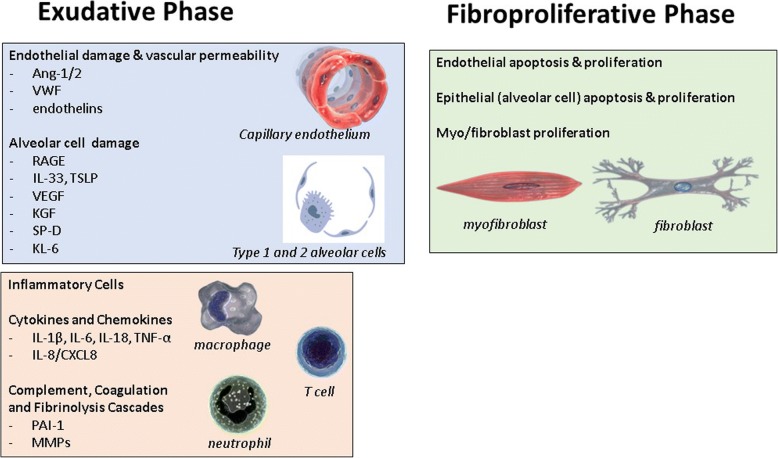
Acute lung injury (ALI) affects over 10% of patients hospitalised in critical care, with acute respiratory distress syndrome (ARDS) being the most severe form of ALI and having a mortality rate in the region of 40%. There has been slow but incremental progress in identification of biomarkers that contribute to the pathophysiology of ARDS, have utility in diagnosis and monitoring, and that are potential therapeutic targets (Calfee CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, Matthay MA, Thompson T, Ware LB, Matthay MA, Lancet Respir Med 2014, 2:611--620). However, a major issue is that ARDS is such a heterogeneous, multi-factorial, end-stage condition that the strategies for "lumping and splitting" are critical (Prescott HC, Calfee CS, Thompson BT, Angus DC, Liu VX, Am J Respir Crit Care Med 2016, 194:147--155). Nevertheless, sequencing of the human genome, the availability of improved methods for analysis of transcription to mRNA (gene expression), and development of sensitive immunoassays has allowed the application of network biology to ARDS, with these biomarkers offering potential for personalised or precision medicine (Sweeney TE, Khatri P, Toward precision medicine Crit Care Med; 2017 45:934-939). Biomarker panels have potential applications in molecular phenotyping for identifying patients at risk of developing ARDS, diagnosis of ARDS, risk stratification and monitoring. Two subphenotypes of ARDS have been identified on the basis of blood biomarkers: hypo-inflammatory and hyper-inflammatory. The hyper-inflammatory subphenotype is associated with shock, metabolic acidosis and worst clinical outcomes. Biomarkers of particular interest have included interleukins (IL-6 and IL-8), interferon gamma (IFN-γ), surfactant proteins (SPD and SPB), von Willebrand factor antigen, angiopoietin 1/2 and plasminogen activator inhibitor-1 (PAI-1). In terms of gene expression (mRNA) in blood there have been found to be increases in neutrophil-related genes in sepsis-induced and influenza-induced ARDS, but whole blood expression does not give a robust diagnostic test for ARDS. Despite improvements in management of ARDS on the critical care unit, this complex disease continues to be a major life-threatening event. Clinical trials of β-agonists, statins, surfactants and keratinocyte growth factor (KGF) have been disappointing. In addition, monoclonal antibodies (anti-TNF) and TNFR fusion protein have also been unconvincing. However, there have been major advances in methods of mechanical ventilation, a neuromuscular blocker (cisatracurium besilate) has shown some benefit, and stem cell therapy is being developed. In the future, by understanding the role of biomarkers in the pathophysiology of ARDS and lung injury, it is hoped that this will provide rational therapeutic targets and ultimately improve clinical care (Seymour CW, Gomez H, Chang CH, Clermont G, Kellum JA, Kennedy J, Yende S, Angus DC, Crit Care 2017, 21:257).
急性肺损伤(ALI)影响着超过10%入住重症监护病房的患者,急性呼吸窘迫综合征(ARDS)是ALI最严重的形式,死亡率约为40%。在有助于ARDS病理生理学、具有诊断和监测效用且为潜在治疗靶点的生物标志物的识别方面,虽进展缓慢但在逐步推进(卡尔菲CS、德卢奇K、帕森斯PE、汤普森BT、韦尔LB、马泰MA、汤普森T、韦尔LB、马泰MA,《柳叶刀呼吸医学》2014年,2:611 - 620)。然而,一个主要问题是ARDS是一种如此异质性、多因素的终末期病症,以至于“合并与细分”策略至关重要(普雷斯科特HC、卡尔菲CS、汤普森BT、安格斯DC、刘VX,《美国呼吸与重症医学杂志》2016年,194:147 - 155)。尽管如此,人类基因组测序、转录至mRNA(基因表达)分析的改进方法的可用性以及灵敏免疫测定的发展,已使网络生物学应用于ARDS,这些生物标志物为个性化或精准医学提供了潜力(斯威尼TE、卡特里P,迈向精准医学,《重症医学》;2017年45:934 - 939)。生物标志物组合在分子表型分析中具有潜在应用,可用于识别有发生ARDS风险的患者、ARDS的诊断、风险分层及监测。基于血液生物标志物已识别出ARDS的两种亚表型:低炎症型和高炎症型。高炎症亚表型与休克、代谢性酸中毒及最差临床结局相关。特别受关注的生物标志物包括白细胞介素(IL - 6和IL - 8)、干扰素γ(IFN - γ)、表面活性蛋白(SPD和SPB)、血管性血友病因子抗原、血管生成素1/2和纤溶酶原激活物抑制剂 - 1(PAI - 1)。就血液中的基因表达(mRNA)而言,在脓毒症诱导和流感诱导的ARDS中已发现中性粒细胞相关基因增加,但全血表达对ARDS并不能提供可靠的诊断检测。尽管重症监护病房对ARDS的管理有所改善,但这种复杂疾病仍然是一个重大的危及生命的事件。β - 激动剂、他汀类药物、表面活性剂和角质形成细胞生长因子(KGF)的临床试验令人失望。此外,单克隆抗体(抗TNF)和TNFR融合蛋白也未令人信服。然而,机械通气方法有了重大进展,一种神经肌肉阻滞剂(苯磺顺阿曲库铵)已显示出一些益处,并且干细胞疗法正在研发中。未来,通过了解生物标志物在ARDS和肺损伤病理生理学中的作用,希望这将提供合理的治疗靶点并最终改善临床护理(西摩CW、戈麦斯H、张CH、克莱蒙特G、凯卢姆JA、肯尼迪J、延德S、安格斯DC,《重症护理》2017年,21:257)