Department of Anaesthesiology and Intensive Care Medicine, University Hospital Ostrava, 708 52 Ostrava, Czech Republic.
Institute of Physiology and Pathophysiology, Faculty of Medicine, University of Ostrava, 703 00 Ostrava, Czech Republic.
Int J Mol Sci. 2022 Jul 29;23(15):8396. doi: 10.3390/ijms23158396.
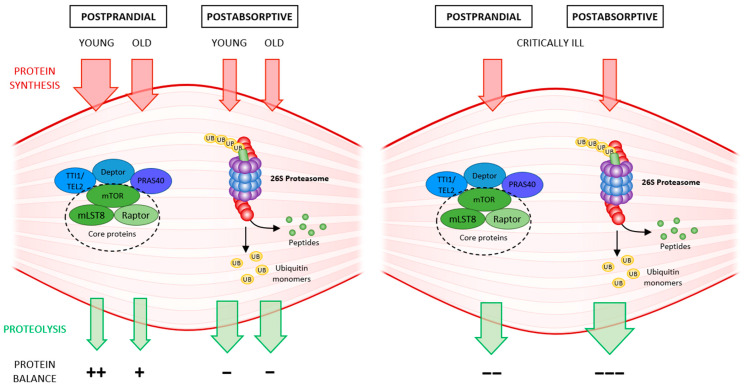
Skeletal muscle is a highly adaptable organ, and its amount declines under catabolic conditions such as critical illness. Aging is accompanied by a gradual loss of muscle, especially when physical activity decreases. Intensive care unit-acquired weakness is a common and highly serious neuromuscular complication in critically ill patients. It is a consequence of critical illness and is characterized by a systemic inflammatory response, leading to metabolic stress, that causes the development of multiple organ dysfunction. Muscle dysfunction is an important component of this syndrome, and the degree of catabolism corresponds to the severity of the condition. The population of critically ill is aging; thus, we face another negative effect-sarcopenia-the age-related decline of skeletal muscle mass and function. Low-grade inflammation gradually accumulates over time, inhibits proteosynthesis, worsens anabolic resistance, and increases insulin resistance. The cumulative consequence is a gradual decline in muscle recovery and muscle mass. The clinical manifestation for both of the above conditions is skeletal muscle weakness, with macromolecular damage, and a common mechanism-mitochondrial dysfunction. In this review, we compare the molecular mechanisms underlying the two types of muscle atrophy, and address questions regarding possible shared molecular mechanisms, and whether critical illness accelerates the aging process.
骨骼肌是一种高度适应性的器官,在分解代谢状态下(如危重病)其数量会减少。衰老伴随着肌肉的逐渐丧失,尤其是当身体活动减少时。重症监护病房获得性肌无力是危重病患者常见且非常严重的神经肌肉并发症。它是危重病的结果,其特征是全身性炎症反应导致代谢应激,从而导致多器官功能障碍。肌肉功能障碍是该综合征的一个重要组成部分,分解代谢的程度与病情的严重程度相对应。危重病患者群体正在老龄化;因此,我们面临着另一个负面影响——肌肉减少症,即与年龄相关的骨骼肌质量和功能下降。低水平炎症会随着时间的推移逐渐积累,抑制蛋白质合成,加重合成代谢抵抗,并增加胰岛素抵抗。累积的结果是肌肉恢复和肌肉质量逐渐下降。这两种情况的临床表现都是骨骼肌无力、大分子损伤和一个共同的机制——线粒体功能障碍。在这篇综述中,我们比较了两种类型的肌肉萎缩的分子机制,并探讨了可能存在的共同分子机制的问题,以及危重病是否会加速衰老过程。