Klawitter Felix, Laukien Friederike, Fischer Dagmar-C, Rahn Anja, Porath Katrin, Danckert Lena, Bajorat Rika, Walter Uwe, Patejdl Robert, Ehler Johannes
Department of Anesthesiology, Intensive Care Medicine, and Pain Therapy, Rostock University Medical Center, Rostock, 18057, Germany.
Department of Pediatrics, Rostock University Medical Center, Rostock, Germany.
Neurocrit Care. 2025 Feb;42(1):118-130. doi: 10.1007/s12028-024-02050-x. Epub 2024 Jul 9.
The diagnosis of intensive care unit (ICU)-acquired weakness (ICUAW) and critical illness neuromyopathy (CINM) is frequently hampered in the clinical routine. We evaluated a novel panel of blood-based inflammatory, neuromuscular, and neurovascular biomarkers as an alternative diagnostic approach for ICUAW and CINM.
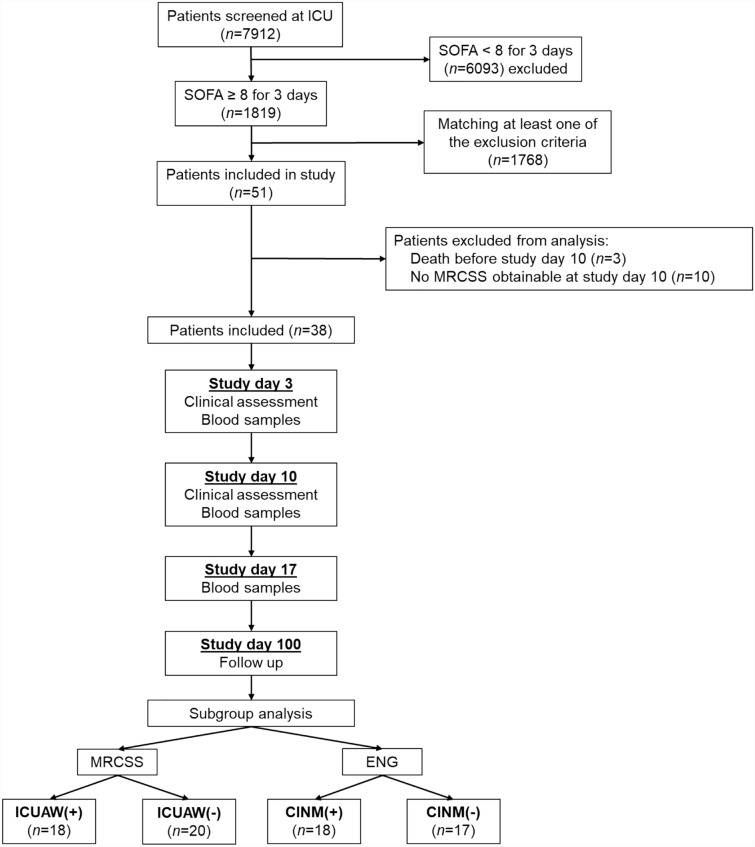
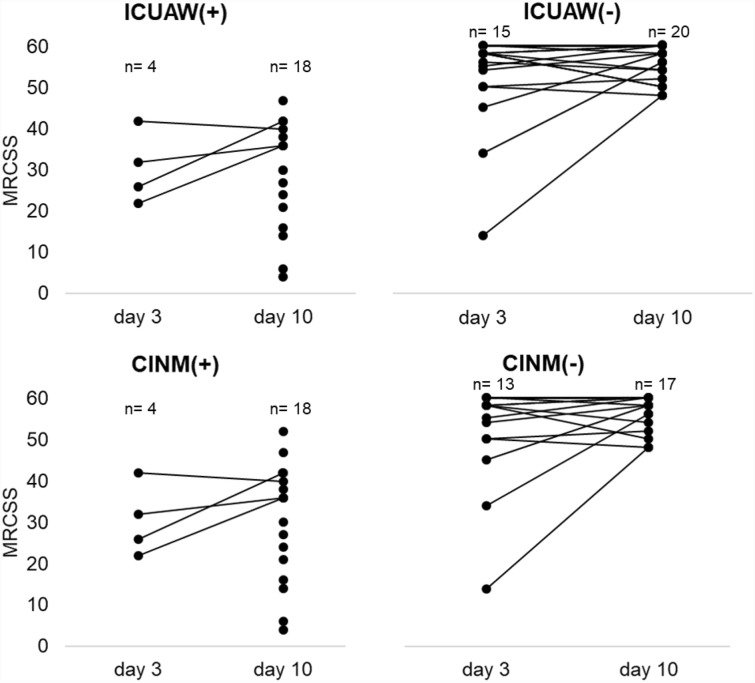
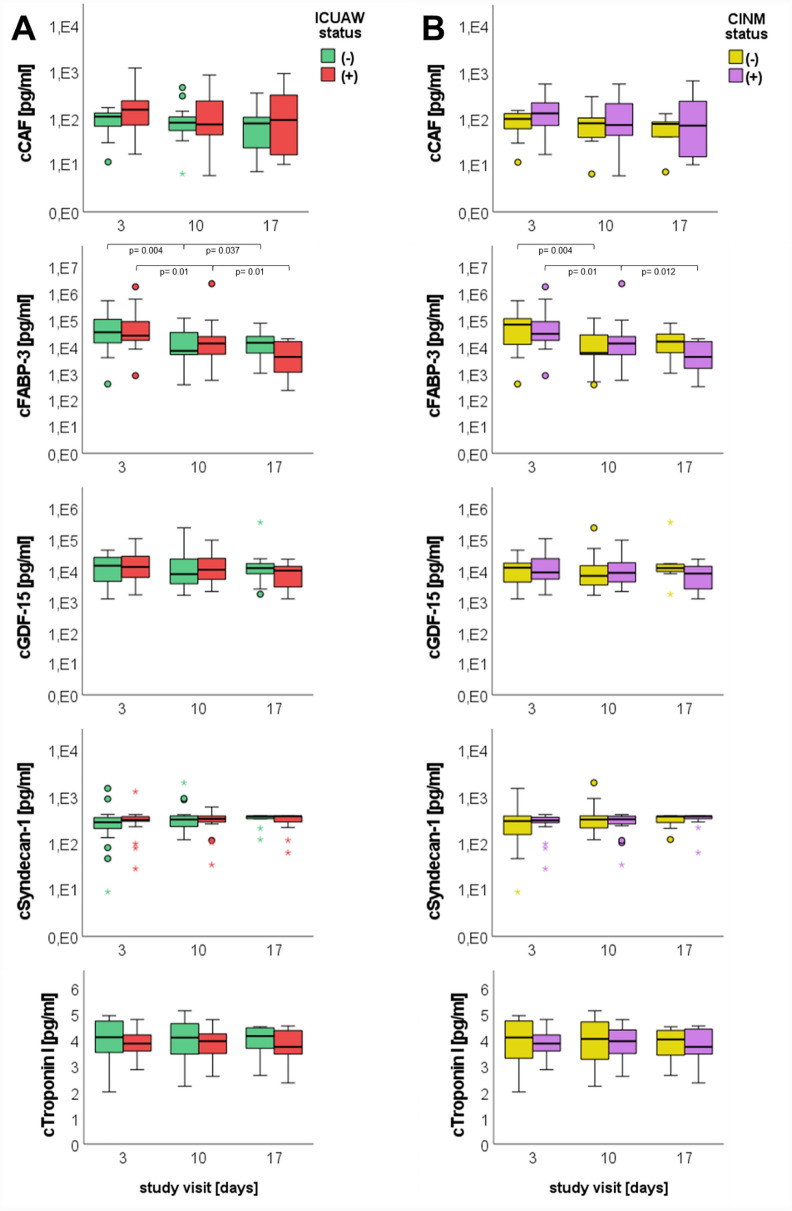
Patients admitted to the ICU with a Sequential Organ Failure Assessment score of ≥ 8 on 3 consecutive days within the first 5 days as well as healthy controls were enrolled. The Medical Research Council Sum Score (MRCSS) was calculated, and motor and sensory electroneurography (ENG) for assessment of peripheral nerve function were performed at days 3 and 10. ICUAW was defined by an MRCSS < 48 and CINM by pathological ENG alterations, both at day 10. Blood samples were taken at days 3, 10, and 17 for quantitative analysis of 18 different biomarkers (white blood cell count, C-reactive protein, procalcitonin, C-terminal agrin filament, fatty-acid-binding protein 3, growth and differentiation factor 15, syndecan 1, troponin I, interferon-γ, tumor necrosis factor-α, interleukin-1α [IL-1α], IL-1β, IL-4, IL-6, IL-8, IL-10, IL-13, and monocyte chemoattractant protein 1). Results of the biomarker analysis were categorized according to the ICUAW and CINM status. Clinical outcome was assessed after 3 months.
Between October 2016 and December 2018, 38 critically ill patients, grouped into ICUAW (18 with and 20 without) and CINM (18 with and 17 without), as well as ten healthy volunteers were included. Biomarkers were significantly elevated in critically ill patients compared to healthy controls and correlated with disease severity and 3-month outcome parameters. However, none of the biomarkers enabled discrimination of patients with and without neuromuscular impairment, irrespective of applied classification.
Blood-based biomarkers are generally elevated in ICU patients but do not identify patients with ICUAW or CINM.
ClinicalTrials.gov identifier: NCT02706314.
在临床实践中,重症监护病房(ICU)获得性肌无力(ICUAW)和危重病性神经病(CINM)的诊断常常受到阻碍。我们评估了一组基于血液的新型炎症、神经肌肉和神经血管生物标志物,作为ICUAW和CINM的一种替代诊断方法。
纳入入住ICU且在最初5天内连续3天序贯器官衰竭评估评分≥8分的患者以及健康对照。计算医学研究委员会总评分(MRCSS),并在第3天和第10天进行运动和感觉神经电图(ENG)检查以评估周围神经功能。ICUAW定义为第10天时MRCSS<48,CINM定义为第10天时ENG出现病理性改变。在第3天、第10天和第17天采集血样,对18种不同生物标志物(白细胞计数、C反应蛋白、降钙素原、C末端集聚蛋白丝、脂肪酸结合蛋白3、生长分化因子15、多配体蛋白聚糖1、肌钙蛋白I、干扰素-γ、肿瘤坏死因子-α、白细胞介素-1α[IL-1α]、IL-1β、IL-4、IL-6、IL-8、IL-10、IL-13和单核细胞趋化蛋白1)进行定量分析。根据ICUAW和CINM状态对生物标志物分析结果进行分类。3个月后评估临床结局。
2016年10月至2018年12月期间,纳入了38例危重病患者,分为ICUAW组(有18例,无20例)和CINM组(有18例,无17例),以及10名健康志愿者。与健康对照相比,危重病患者的生物标志物显著升高,且与疾病严重程度和3个月结局参数相关。然而,无论采用何种分类方法,没有一种生物标志物能够区分有无神经肌肉损伤的患者。
基于血液的生物标志物在ICU患者中通常会升高,但无法识别患有ICUAW或CINM的患者。
ClinicalTrials.gov标识符:NCT02706314。