Department of Anesthesiology, University of Michigan Medical School, Ann Arbor, Michigan; Center for Consciousness Science, University of Michigan Medical School, Ann Arbor, Michigan.
Department of Anesthesiology, University of Michigan Medical School, Ann Arbor, Michigan.
Anesthesiology. 2022 Oct 1;137(4):434-445. doi: 10.1097/ALN.0000000000004354.
The relationship between intraoperative physiology and postoperative stroke is incompletely understood. Preliminary data suggest that either hypo- or hypercapnia coupled with reduced cerebrovascular inflow (e.g., due to hypotension) can lead to ischemia. This study tested the hypothesis that the combination of intraoperative hypotension and either hypo- or hypercarbia is associated with postoperative ischemic stroke.
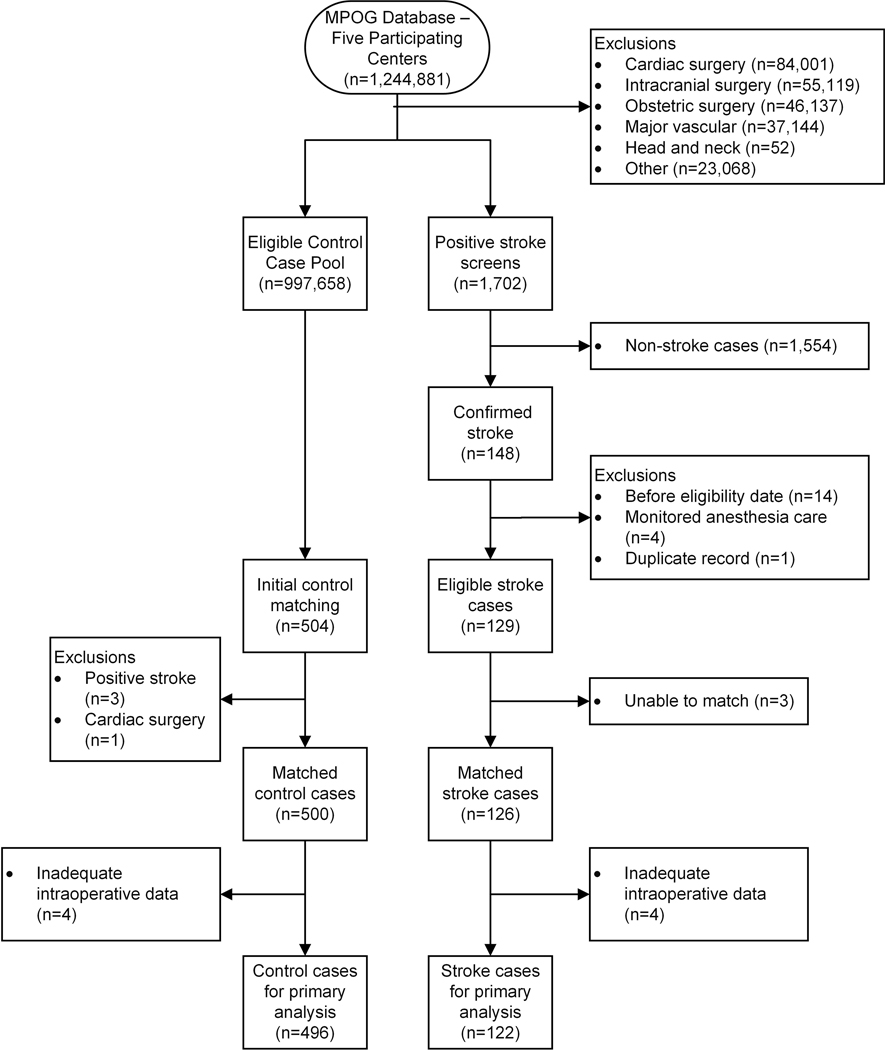
We conducted a retrospective, case-control study via the Multicenter Perioperative Outcomes Group. Noncardiac, nonintracranial, and nonmajor vascular surgical cases (18 yr or older) were extracted from five major academic centers between January 2004 and December 2015. Ischemic stroke cases were identified via manual chart review and matched to controls (1:4). Time and reduction below key mean arterial blood pressure thresholds (less than 55 mmHg, less than 60 mmHg, less than 65 mmHg) and outside of specific end-tidal carbon dioxide thresholds (30 mmHg or less, 35 mmHg or less, 45 mmHg or greater) were calculated based on total area under the curve. The association between stroke and total area under the curve values was then tested while adjusting for relevant confounders.
In total, 1,244,881 cases were analyzed. Among the cases that screened positive for stroke (n = 1,702), 126 were confirmed and successfully matched with 500 corresponding controls. Total area under the curve was significantly associated with stroke for all thresholds tested, with the strongest combination observed with mean arterial pressure less than 55 mmHg (adjusted odds ratio per 10 mmHg-min, 1.17 [95% CI, 1.10 to 1.23], P < 0.0001) and end-tidal carbon dioxide 45 mmHg or greater (adjusted odds ratio per 10 mmHg-min, 1.11 [95% CI, 1.10 to 1.11], P < 0.0001). There was no interaction effect observed between blood pressure and carbon dioxide.
Intraoperative hypotension and carbon dioxide dysregulation may each independently increase postoperative stroke risk.
术中生理学与术后卒中之间的关系尚未完全阐明。初步数据表明,低碳酸血症或高碳酸血症与脑血流减少(例如由于低血压)结合可导致缺血。本研究检验了这样一个假设,即术中低血压与低碳酸血症或高碳酸血症的组合与术后缺血性卒中相关。
我们通过多中心围手术期结局组进行了回顾性病例对照研究。从 2004 年 1 月至 2015 年 12 月,从五个主要学术中心提取了非心脏、非颅内和非主要血管手术(18 岁或以上)病例。通过手动图表审查确定缺血性卒中病例,并与对照组(1:4)匹配。根据总曲线下面积计算时间和关键平均动脉血压阈值以下(低于 55mmHg,低于 60mmHg,低于 65mmHg)和特定呼气末二氧化碳阈值以外(30mmHg 或以下,35mmHg 或以下,45mmHg 或以上)的时间和降低幅度。然后,在调整相关混杂因素后,测试卒中与总曲线下面积值之间的关联。
共分析了 1244881 例病例。在筛选出卒中阳性的病例中(n=1702),有 126 例得到证实,并成功与 500 例相应的对照组匹配。所有测试的阈值下,总曲线下面积与卒中显著相关,在平均动脉压低于 55mmHg(调整后的每 10mmHg-min 优势比,1.17[95%置信区间,1.10 至 1.23],P<0.0001)和呼气末二氧化碳 45mmHg 或更高(调整后的每 10mmHg-min 优势比,1.11[95%置信区间,1.10 至 1.11],P<0.0001)时观察到最强的组合。未观察到血压和二氧化碳之间的相互作用效应。
术中低血压和二氧化碳失调可能各自独立增加术后卒中风险。