From the Department of Anesthesiology, University of Michigan Medical School, Ann Arbor, Michigan.
Department of Anesthesiology, Medical College of Wisconsin, Milwaukee, Wisconsin.
Anesth Analg. 2020 May;130(5):1133-1146. doi: 10.1213/ANE.0000000000004489.
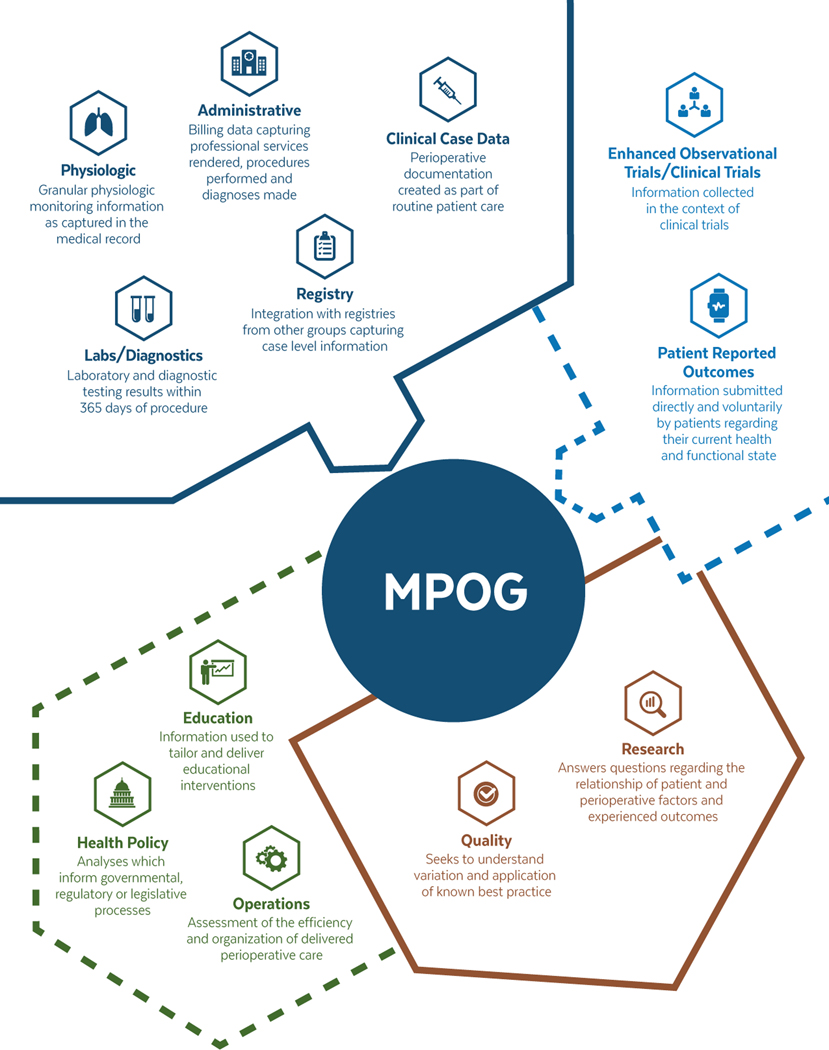
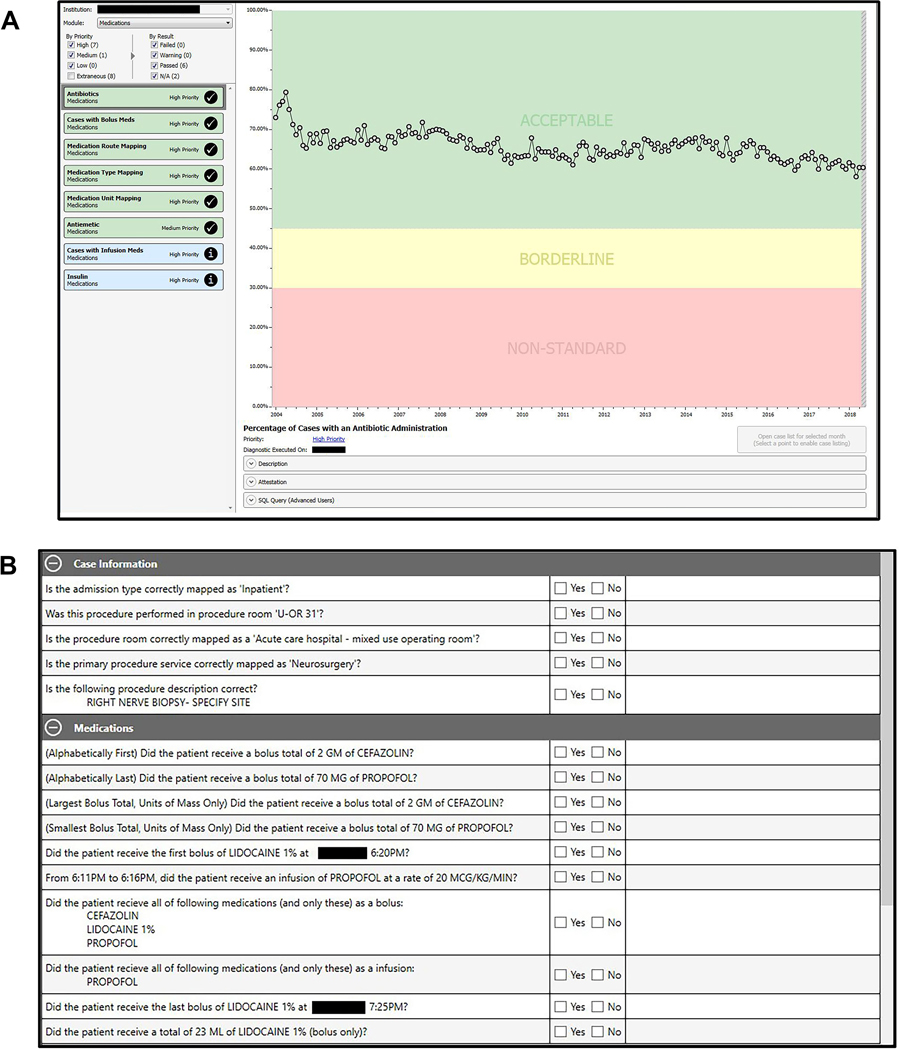
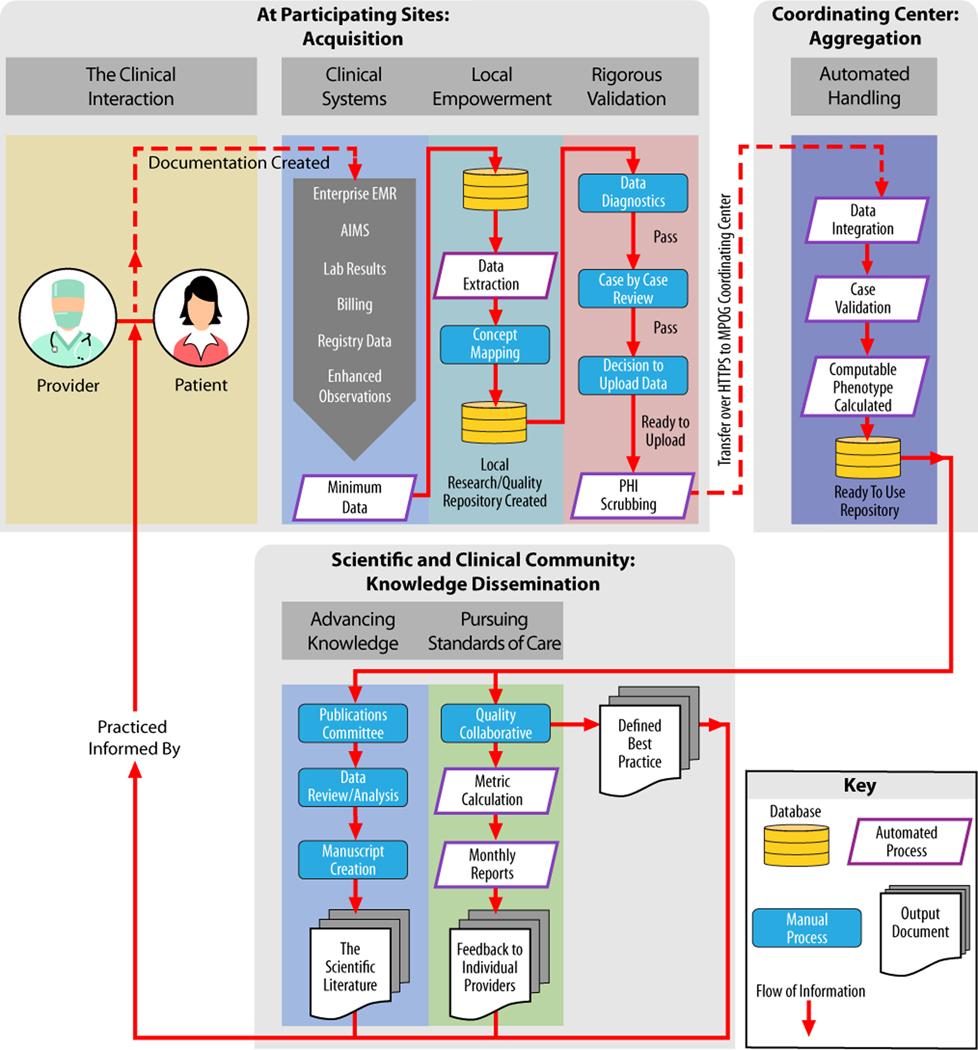
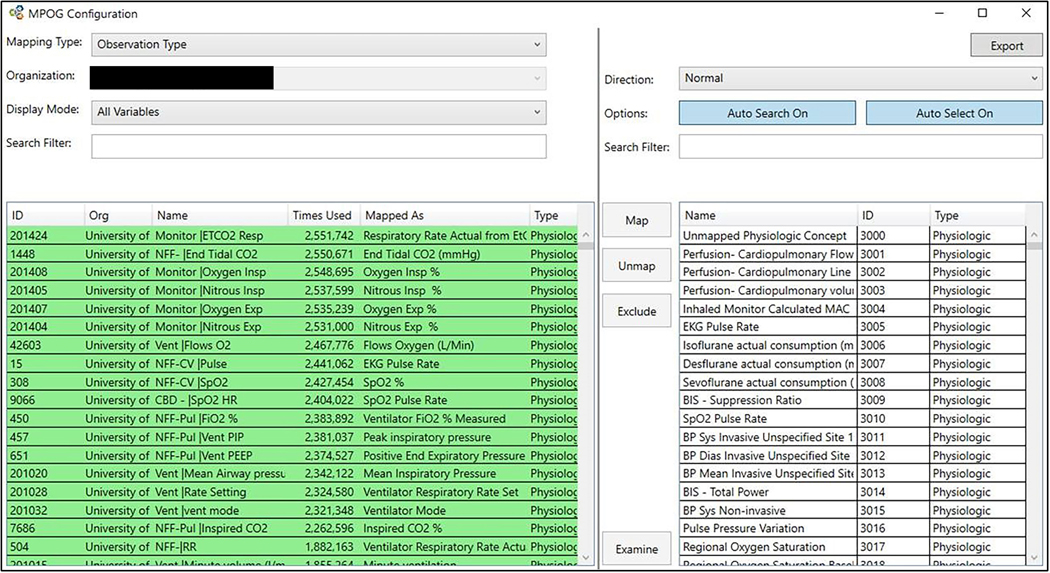
Use of the electronic health record (EHR) has become a routine part of perioperative care in the United States. Secondary use of EHR data includes research, quality, and educational initiatives. Fundamental to secondary use is a framework to ensure fidelity, transparency, and completeness of the source data. In developing this framework, competing priorities must be considered as to which data sources are used and how data are organized and incorporated into a useable format. In assembling perioperative data from diverse institutions across the United States and Europe, the Multicenter Perioperative Outcomes Group (MPOG) has developed methods to support such a framework. This special article outlines how MPOG has approached considerations of data structure, validation, and accessibility to support multicenter integration of perioperative EHRs. In this multicenter practice registry, MPOG has developed processes to extract data from the perioperative EHR; transform data into a standardized format; and validate, deidentify, and transfer data to a secure central Coordinating Center database. Participating institutions may obtain access to this central database, governed by quality and research committees, to inform clinical practice and contribute to the scientific and clinical communities. Through a rigorous and standardized approach to ensure data integrity, MPOG enables data to be usable for quality improvement and advancing scientific knowledge. As of March 2019, our collaboration of 46 hospitals has accrued 10.7 million anesthesia records with associated perioperative EHR data across heterogeneous vendors. Facilitated by MPOG, each site retains access to a local repository containing all site-specific perioperative data, distinct from source EHRs and readily available for local research, quality, and educational initiatives. Through committee approval processes, investigators at participating sites may additionally access multicenter data for similar initiatives. Emerging from this work are 4 considerations that our group has prioritized to improve data quality: (1) data should be available at the local level before Coordinating Center transfer; (2) data should be rigorously validated against standardized metrics before use; (3) data should be curated into computable phenotypes that are easily accessible; and (4) data should be collected for both research and quality improvement purposes because these complementary goals bolster the strength of each endeavor.
在美国,电子健康记录(EHR)的使用已成为围手术期护理的常规部分。EHR 数据的二次使用包括研究、质量和教育计划。二次使用的基础是一个确保源数据的保真度、透明度和完整性的框架。在制定这个框架时,必须考虑到哪些数据源被使用以及如何组织和整合数据以形成可用格式等竞争优先级。在从美国和欧洲的不同机构收集围手术期数据时,多中心围手术期结局小组(MPOG)已经开发了支持此类框架的方法。这篇特别文章概述了 MPOG 如何处理数据结构、验证和可访问性的考虑因素,以支持围手术期 EHR 的多中心整合。在这个多中心实践注册中心,MPOG 已经开发了从围手术期 EHR 中提取数据的过程;将数据转换为标准化格式;验证、去识别并将数据传输到安全的中央协调中心数据库。参与机构可以通过质量和研究委员会获得对该中央数据库的访问,以告知临床实践并为临床和科学界做出贡献。通过一种严格和标准化的方法来确保数据完整性,MPOG 使数据能够用于质量改进和推进科学知识。截至 2019 年 3 月,我们的 46 家合作医院已经积累了 1070 万例麻醉记录,以及来自不同供应商的相关围手术期 EHR 数据。通过 MPOG 的协助,每个站点都可以访问包含所有特定于站点的围手术期数据的本地存储库,这些数据与源 EHR 不同,并且可随时用于本地研究、质量和教育计划。通过委员会批准程序,参与站点的研究人员可以另外访问用于类似计划的多中心数据。通过这项工作,我们小组确定了 4 个优先事项来提高数据质量:(1)在协调中心转移之前,数据应在本地可用;(2)在使用之前,数据应严格按照标准化指标进行验证;(3)数据应整理成易于访问的可计算表型;(4)应收集数据用于研究和质量改进目的,因为这些互补目标可以增强每项工作的强度。