Gao Xiangcheng, Du Jinpeng, Gao Lin, Hao Dingjun, Hui Hua, He Baorong, Yan Liang
Department of Spine Surgery, Honghui Hospital, Xi'an Jiaotong University, Xi'an, China.
Medical College, Yan'an University, Yan'an, China.
Front Surg. 2022 Jul 28;9:947212. doi: 10.3389/fsurg.2022.947212. eCollection 2022.
To explore the risk factors of bone cement displacement after percutaneous vertebral augmentation (PVA) in patients with osteoporotic vertebral compression fracture (OVCF).
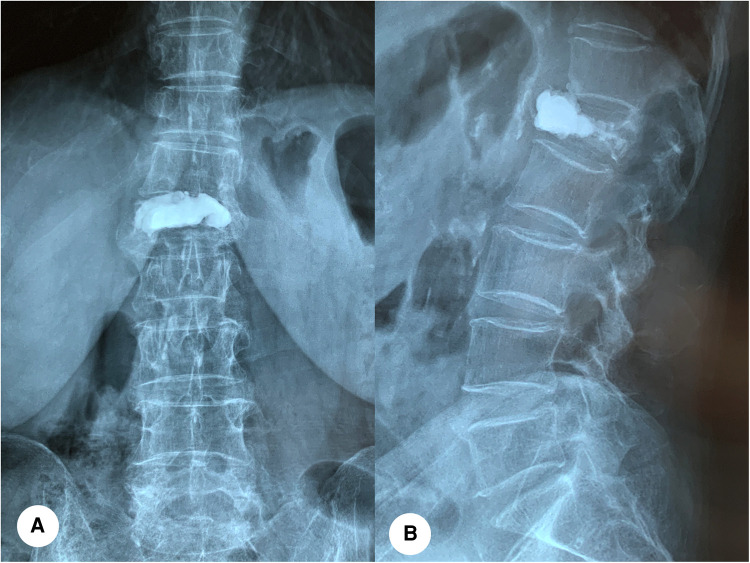
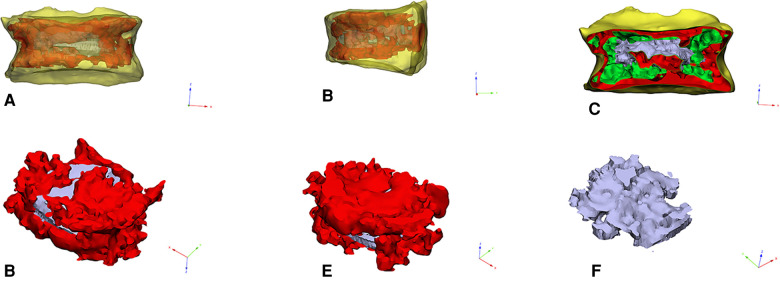
We retrospectively reviewed the records of 1,538 patients with OVCF treated with percutaneous vertebroplasty (PVP) or percutaneous vertebroplasty (PKP) from January 2016 to June 2021. Patients were divided into bone cement displacement group (= 78) and bone cement non-displacement group (= 1,460) according to the radiographic images. Possible risk factors for bone cement displacement were noted, including age, gender, body mass index (BMI), bone mineral density (BMD), underlying disease, number of fractured vertebrae, involved vertebral segment, surgical method, surgical approach, vertebral height, Cobb angle, cement leakage, the viscosity of bone cement, bone cement diffuse ratio, degree of bone cement interweaving, sagittal bone cement placement, targeted location of bone cement, the distance between the bone cement and the upper and lower endplates, the time of wearing brace and postoperative osteoporosis treatment. Risk factors were identified with univariate and multivariate logistic regressions and the discrimination ability of the predictive indicators was evaluated using area under the curve (AUC) of the receiver operating characteristic (ROC).
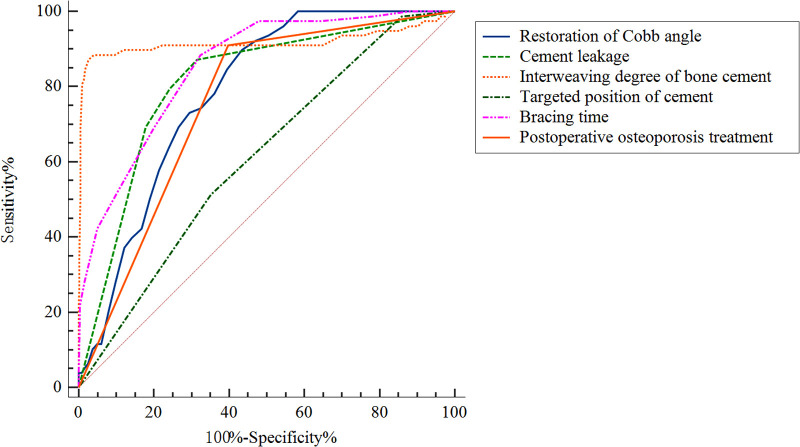
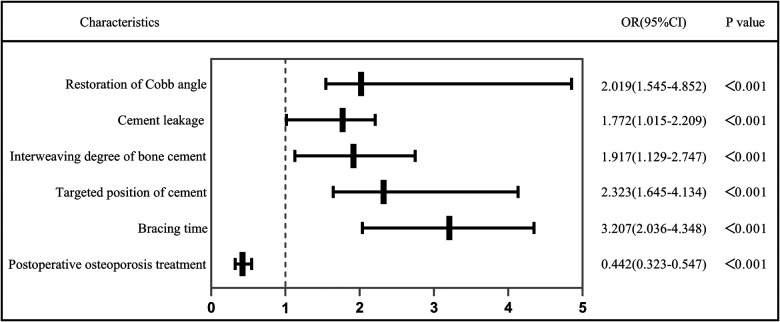
In multivariate regression, independent risk factors for bone cement displacement included: high restoration of Cobb angle (OR = 2.019, 95%[CI] 1.545-4.852, < 0.001), cement leakage (anterior edge) (OR = 1.727, 95%[CI] 1.05-2.20, < 0.001), small degree of bone cement interweaving (OR = 1.917, 95%[CI] 1.129-2.747, < 0.001), non-targeted location of bone cement (OR = 2.323, 95%[CI] 1.645-4.134, < 0.001), short duration of brace wearing (OR = 3.207, 95%[CI] 2.036-4.348, < 0.001) and postoperative osteoporosis treatment (OR = 0.422, 95% CI = 0.323-0.547, < 0.001). The AUCs for the high restoration of Cobb angle, cement leakage (anterior edge), small degree of bone cement interweaving, non-targeted location of bone cement, short duration of brace wearing and non-postoperative osteoporosis treatment were 0.784 (95% CI, 0.747-0.821), 0.811 (95% CI 0.764-0.859), 0.917 (95%CI 0.864-0.970), 0.610 (95%CI 0.552-0.669), 0.854 (95%CI 0.816-0.892) and 0.756 (95% CI, 0.712-0.800), respectively.
High restoration of Cobb angle, cement leakage (anterior edge), small degree of bone cement interweaving, non-targeted location of bone cement, short duration of brace wearing and non-postoperative osteoporosis treatment were the independent risk factors of bone cement displacement after PVA.
探讨骨质疏松性椎体压缩骨折(OVCF)患者经皮椎体强化术(PVA)后骨水泥移位的危险因素。
回顾性分析2016年1月至2021年6月间1538例行经皮椎体成形术(PVP)或经皮后凸成形术(PKP)治疗的OVCF患者的病历资料。根据影像学图像将患者分为骨水泥移位组(n = 78)和骨水泥未移位组(n = 1460)。记录可能导致骨水泥移位的危险因素,包括年龄、性别、体重指数(BMI)、骨密度(BMD)、基础疾病、骨折椎体数量、受累椎体节段、手术方式、手术入路、椎体高度、Cobb角、骨水泥渗漏、骨水泥黏度、骨水泥弥散率、骨水泥交织程度、矢状位骨水泥置入情况、骨水泥靶向位置、骨水泥与上下终板的距离、佩戴支具时间及术后骨质疏松治疗情况。采用单因素和多因素逻辑回归分析确定危险因素,并使用受试者工作特征(ROC)曲线下面积(AUC)评估预测指标的判别能力。
多因素回归分析显示,骨水泥移位的独立危险因素包括:Cobb角恢复程度高(OR = 2.019,95%[CI] 1.545 - 4.852,P < 0.001)、骨水泥渗漏(前缘)(OR = 1.727,95%[CI] 1.05 - 2.20,P < 0.001)、骨水泥交织程度小(OR = 1.917,95%[CI] 1.129 - 2.747,P < 0.001)、骨水泥非靶向位置(OR = 2.323,95%[CI] 1.645 - 4.134,P < 0.001)、佩戴支具时间短(OR = 3.207,95%[CI] 2.036 - 4.348,P < 0.001)及术后骨质疏松治疗(OR = 0.422,95% CI = 0.323 - 0.547,P < 0.001)。Cobb角恢复程度高、骨水泥渗漏(前缘)、骨水泥交织程度小、骨水泥非靶向位置、佩戴支具时间短及未进行术后骨质疏松治疗的AUC分别为0.784(95% CI,0.747 - 0.821)、0.811(95% CI 0.764 - 0.859)、0.917(95%CI 0.864 - 0.970)、0.610(95%CI 0.552 - 0.669)、0.854(95%CI 0.816 - 0.892)和0.756(95% CI,0.712 - 0.800)。
Cobb角恢复程度高、骨水泥渗漏(前缘)、骨水泥交织程度小、骨水泥非靶向位置、佩戴支具时间短及未进行术后骨质疏松治疗是PVA后骨水泥移位的独立危险因素。