Department of Cardiology, Medical Center Groningen, University of Groningen, Antonius Deusinglaan 1, PO Box 30.001, 9700 RB, Groningen, the Netherlands.
Department of Social and Welfare Studies, Linköping University, Linköping, Sweden.
Clin Res Cardiol. 2023 Jan;112(1):123-133. doi: 10.1007/s00392-022-02076-1. Epub 2022 Aug 17.
Management of comorbidities represents a critical step in optimal treatment of heart failure (HF) patients. However, minimal attention has been paid whether comorbidity burden and their prognostic value changes over time. Therefore, we examined the association between comorbidities and clinical outcomes in HF patients between 2002 and 2017.
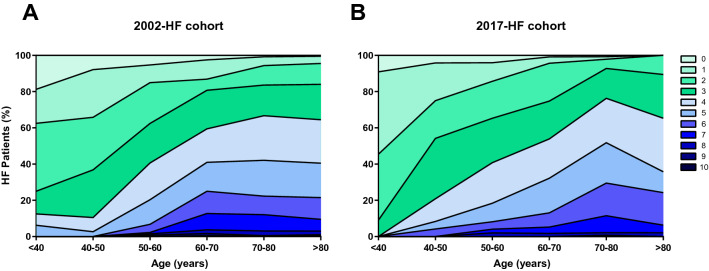
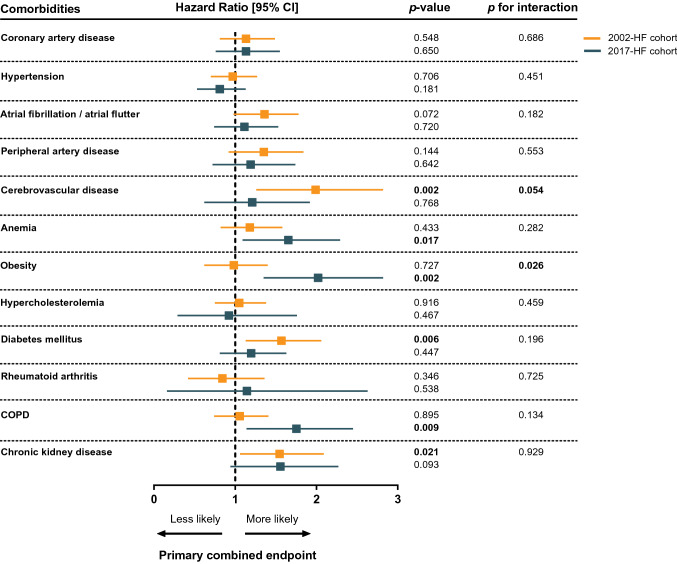
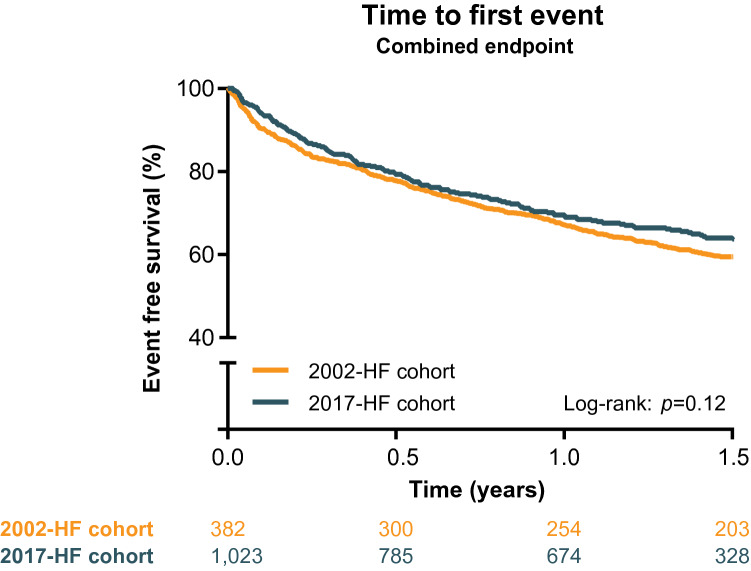
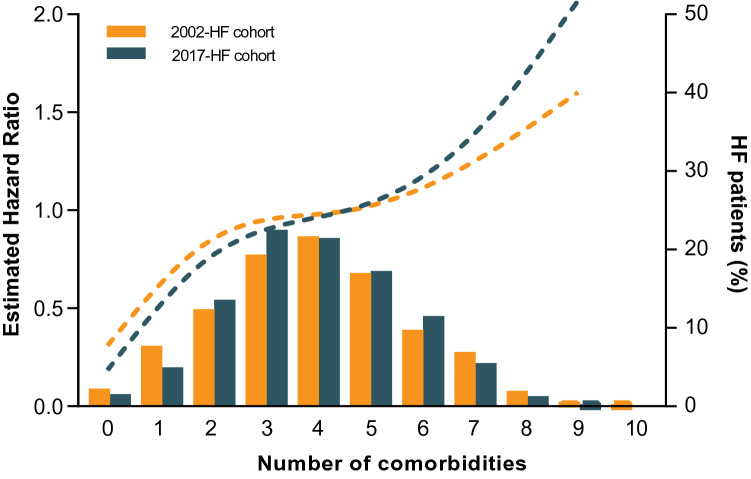
The 2002-HF cohort consisted of patients from The Coordinating Study Evaluating Outcomes of Advising and Counseling in Heart Failure (COACH) trial (n = 1,032). The 2017-HF cohort were outpatient HF patients enrolled after hospitalization for HF in a tertiary referral academic hospital (n = 382). Kaplan meier and cox regression analyses were used to assess the association of comorbidities with HF hospitalization and all-cause mortality. Patients from the 2017-cohort were more likely to be classified as HF with preserved ejection fraction (24 vs 15%, p < 0.001), compared to patients from the 2002-cohort. Comorbidity burden was comparable between both cohorts (mean of 3.9 comorbidities per patient) and substantially increased with age. Higher comorbidity burden was significantly associated with a comparable increased risk for HF hospitalization and all-cause mortality (HR 1.12 [1.02-1.22] and HR 1.18 [1.05-1.32]), in the 2002- and 2017-cohort respectively. When assessing individual comorbidities, obesity yielded a statistically higher prognostic effect on outcome in the 2017-cohort compared to the 2002-HF cohort (p for interaction 0.026).
Despite major advances in HF treatment over the past decades, comorbidity burden remains high in HF and influences outcome to a large extent. Obesity emerges as a prominent comorbidity, and efforts should be made for prevention and treatment. Created with BioRender.com.
合并症的管理是心力衰竭(HF)患者最佳治疗的关键步骤。然而,几乎没有关注合并症负担及其预后价值是否随时间而变化。因此,我们研究了 2002 年至 2017 年间 HF 患者合并症与临床结局之间的关系。
2002-HF 队列包括来自协调研究评估心力衰竭咨询和辅导结局(COACH)试验的患者(n=1032)。2017-HF 队列是在一家三级转诊学术医院因 HF 住院后登记的门诊 HF 患者(n=382)。Kaplan-Meier 和 Cox 回归分析用于评估合并症与 HF 住院和全因死亡率的关系。与 2002 队列相比,2017 队列的患者更有可能被归类为射血分数保留的 HF(24%比 15%,p<0.001)。两个队列的合并症负担相当(每位患者平均 3.9 种合并症),并随年龄增长而显著增加。在 2002 队列和 2017 队列中,更高的合并症负担与 HF 住院和全因死亡率的风险增加显著相关(HR 1.12[1.02-1.22]和 HR 1.18[1.05-1.32])。在评估个别合并症时,肥胖在 2017 队列中的预后效果比 2002-HF 队列更高(p 交互=0.026)。
尽管 HF 治疗在过去几十年取得了重大进展,但 HF 患者的合并症负担仍然很高,对结局有很大影响。肥胖成为突出的合并症,应努力预防和治疗。由 BioRender.com 创建。