Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, UK.
Leeds Institute of Health Sciences, University of Leeds, Leeds, UK.
Heart. 2021 Sep;107(17):1417-1421. doi: 10.1136/heartjnl-2020-317833. Epub 2020 Nov 5.
Estimating survival can aid care planning, but the use of absolute survival projections can be challenging for patients and clinicians to contextualise. We aimed to define how heart failure and its major comorbidities contribute to loss of actuarially predicted life expectancy.
We conducted an observational cohort study of 1794 adults with stable chronic heart failure and reduced left ventricular ejection fraction, recruited from cardiology outpatient departments of four UK hospitals. Data from an 11-year maximum (5-year median) follow-up period (999 deaths) were used to define how heart failure and its major comorbidities impact on survival, relative to an age-sex matched control UK population, using a relative survival framework.
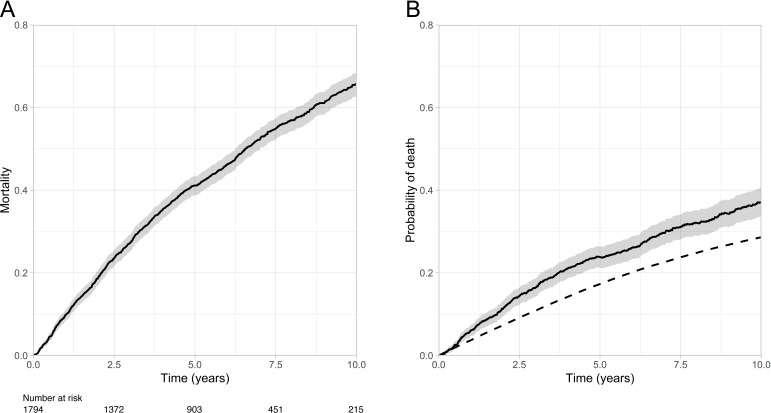
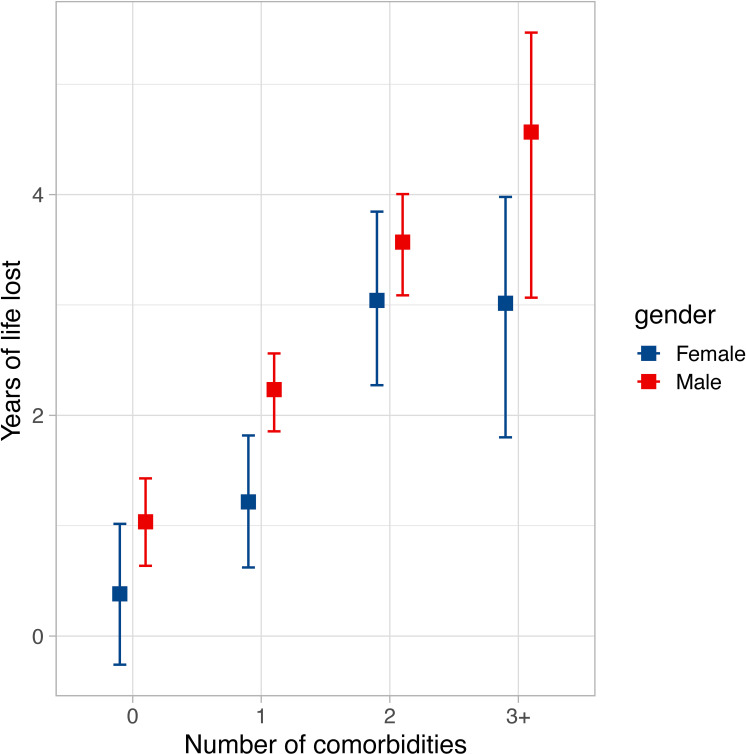
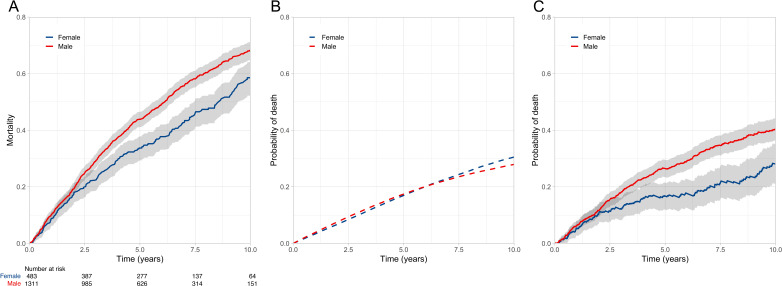
After 10 years, mortality in the reference control population was 29%. In people with heart failure, this increased by an additional 37% (95% CI 34% to 40%), equating to an additional 2.2 years of lost life or a 2.4-fold (2.2-2.5) excess loss of life. This excess was greater in men than women (2.4 years (2.2-2.7) vs 1.6 years (1.2-2.0); p<0.001). In patients without major comorbidity, men still experienced excess loss of life, while women experienced less and were non-significantly different from the reference population (1 year (0.6-1.5) vs 0.4 years (-0.3 to 1); p<0.001). Accrual of comorbidity was associated with substantial increases in excess lost life, particularly for diabetes, chronic kidney and lung disease.
Comorbidity accounts for the majority of lost life expectancy in people with heart failure. Women, but not men, without comorbidity experience survival close to reference controls.
评估生存率有助于制定护理计划,但患者和临床医生难以理解绝对生存率预测值的具体情况。本研究旨在明确心力衰竭及其主要合并症如何导致预期寿命的损失。
我们对来自四家英国医院心内科门诊的 1794 名射血分数降低的稳定慢性心力衰竭成人患者进行了一项观察性队列研究。使用 11 年(中位随访 5 年)的最大随访数据(999 例死亡),采用相对生存率框架,定义心力衰竭及其主要合并症对生存率的影响相对于年龄性别匹配的英国对照人群。
10 年后,参照对照人群的死亡率为 29%。心力衰竭患者的死亡率增加了 37%(95%CI 34%至 40%),相当于额外损失了 2.2 年的生命或 2.4 倍(2.2-2.5)的超额生命损失。男性的超额死亡率高于女性(2.4 年(2.2-2.7)比 1.6 年(1.2-2.0);p<0.001)。在无主要合并症的患者中,男性仍然存在超额生命损失,而女性的超额生命损失较少,与参照人群无显著差异(1 年(0.6-1.5)比 0.4 年(-0.3 至 1);p<0.001)。合并症的发生与超额生命损失的显著增加有关,尤其是糖尿病、慢性肾脏病和肺部疾病。
合并症是心力衰竭患者预期寿命损失的主要原因。无合并症的女性,而不是男性,其生存率接近参照人群。