Department of Health Services Research and Policy, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Department of Health Services and Population Research, King's College London, London, United Kingdom.
PLoS One. 2022 Aug 17;17(8):e0272854. doi: 10.1371/journal.pone.0272854. eCollection 2022.
The INTERVAL trial showed shorter inter-donation intervals could safely increase the frequency of whole-blood donation. We extended the INTERVAL trial to consider the relative cost-effectiveness of reduced inter-donation intervals.
Our within-trial cost-effectiveness analysis (CEA) used data from 44,863 whole-blood donors randomly assigned to 12, 10 or 8 week (males), and 16, 14 or 12 week inter-donation intervals (females). The CEA analysed the number of whole-blood donations, deferrals including low- haemoglobin deferrals, and donors' health-related quality of life (QoL) to report costs and cost-effectiveness over two years.
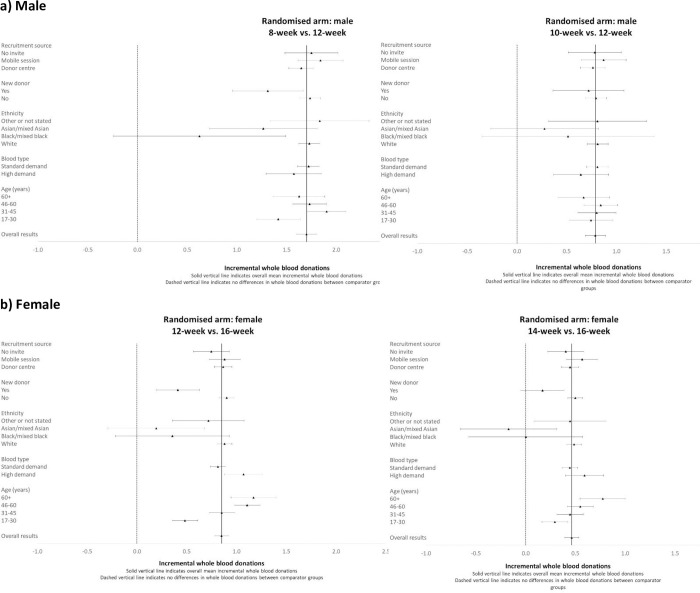
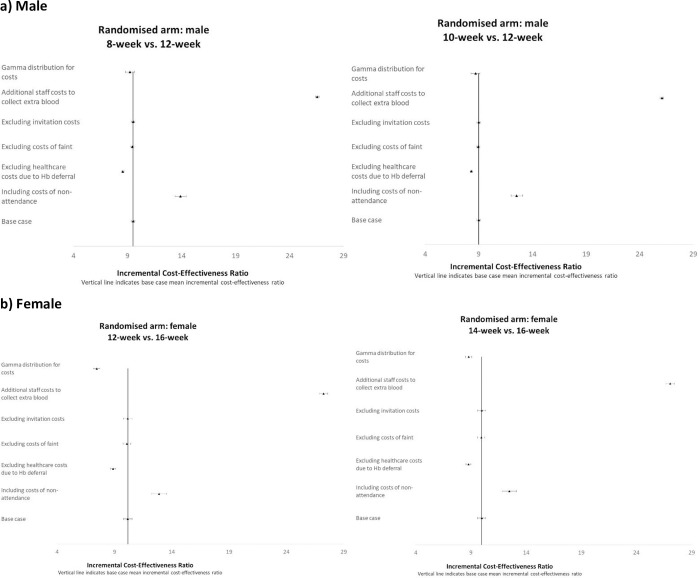
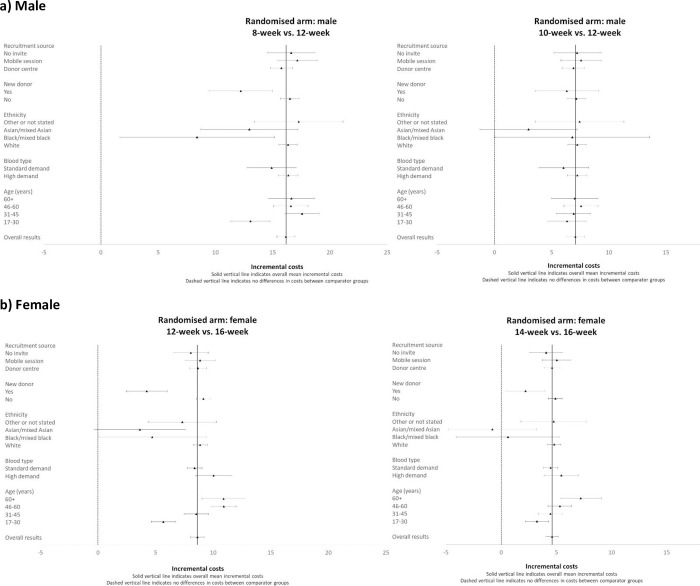
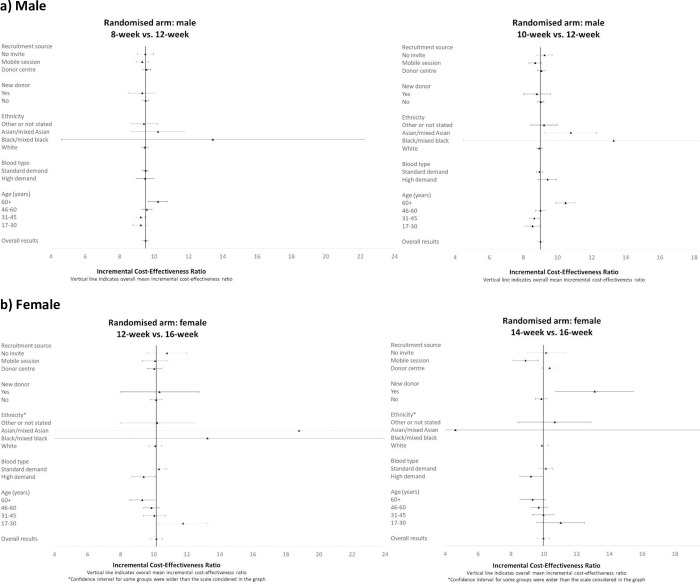
The mean number of blood donation visits over two years was higher for the reduced interval strategies, for males (7.76, 6.60 and 5.68 average donations in the 8-, 10- and 12- week arms) and for females (5.10, 4.60 and 4.01 donations in the 12-, 14- and 16- week arms). For males, the average rate of deferral for low haemoglobin per session attended, was 5.71% (8- week arm), 3.73% (10- week), and 2.55% (12- week), and for females the rates were: 7.92% (12-week), 6.63% (14- week), and 5.05% (16- week). Donors' QoL was similar across strategies, although self-reported symptoms were increased with shorter donation intervals. The shorter interval strategies increased average cost, with incremental cost-effectiveness ratios of £9.51 (95% CI 9.33 to 9.69) per additional whole-blood donation for the 8- versus 12- week interval for males, and £10.17 (95% CI 9.80 to 10.54) for the 12- versus 16- week interval arm for females.
Over two years, reducing the minimum donation interval could provide additional units of whole-blood at a small additional cost, including for those donor subgroups whose blood type is in relatively high demand. However, the significance of self-reported symptoms needs to be investigated further before these policies are expanded.
INTERVAL 试验表明,缩短供者间间隔时间可安全地增加全血捐献频率。我们对 INTERVAL 试验进行了扩展,以考虑缩短供者间间隔时间的相对成本效益。
我们的试验内成本效益分析(CEA)使用了来自 44863 名全血供者的数据,这些供者被随机分配至 12 周、10 周或 8 周(男性)以及 16 周、14 周或 12 周的供者间间隔时间(女性)。CEA 分析了全血捐献次数、包括低血红蛋白捐献在内的延期情况以及供者的健康相关生活质量(QoL),以报告两年内的成本和成本效益。
对于缩短间隔策略,男性(8 周、10 周和 12 周组的平均献血次数分别为 7.76、6.60 和 5.68)和女性(12 周、14 周和 16 周组的平均献血次数分别为 5.10、4.60 和 4.01)的两年内平均献血就诊次数更高。对于男性,每次就诊低血红蛋白的平均延期率为 5.71%(8 周组)、3.73%(10 周组)和 2.55%(12 周组),而对于女性,该比率分别为:7.92%(12 周组)、6.63%(14 周组)和 5.05%(16 周组)。尽管随着供者间间隔时间缩短,自我报告的症状有所增加,但供者的 QoL 在各策略间相似。缩短间隔策略增加了平均成本,对于男性,8 周与 12 周组间的增量成本效益比为每增加一次全血捐献需额外支付 9.51 英镑(95%CI 9.33 至 9.69),对于女性,12 周与 16 周组间的增量成本效益比为每增加一次全血捐献需额外支付 10.17 英镑(95%CI 9.80 至 10.54)。
在两年内,缩短最低供者间间隔时间可以在增加少量额外成本的情况下提供更多单位的全血,包括对那些血液需求量相对较高的供者亚组。然而,在扩大这些政策之前,需要进一步调查自我报告症状的意义。