Center for Surgery and Public Health, Brigham and Women's Hospital, Boston, Massachusetts.
Cornell Center for Research on End-of-Life Care, Weill Cornell Medicine, New York, New York.
JAMA Health Forum. 2021 Jul 30;2(7):e211829. doi: 10.1001/jamahealthforum.2021.1829. eCollection 2021 Jul.
Advance care planning (ACP) is intended to maximize the concordance of preferences with end-of-life (EOL) care and is assumed to lead to less intensive use of health care services. The Centers for Medicare & Medicaid Services began reimbursing clinicians for ACP discussions with patients in 2016.
To determine whether billed ACP visits are associated with intensive use of health care services at EOL.
This prospective patient-level cohort analysis of seriously ill patients included Medicare fee-for-service beneficiaries who met criteria for serious illness from January 1 to December 31, 2016, and died from January 1, 2017, to December 31, 2018. Analyses were completed from November 1, 2020, to March 31, 2021.
Five measures of EOL health care services used (inpatient admission, emergency department visit, and/or intensive care unit stay within 30 days of death; in-hospital death; and timing of first hospice bill) and a measure of EOL expenditures. Analyses were adjusted for age, race and ethnicity, sex, Charlson Comorbidity Index, Medicare-Medicaid dual eligibility, and expenditure by hospital referral region (high, medium, or low). The primary exposure was receipt of a billed ACP service classified as none, timely (>1 month before death), or late (first ACP visit ≤1 month before death).
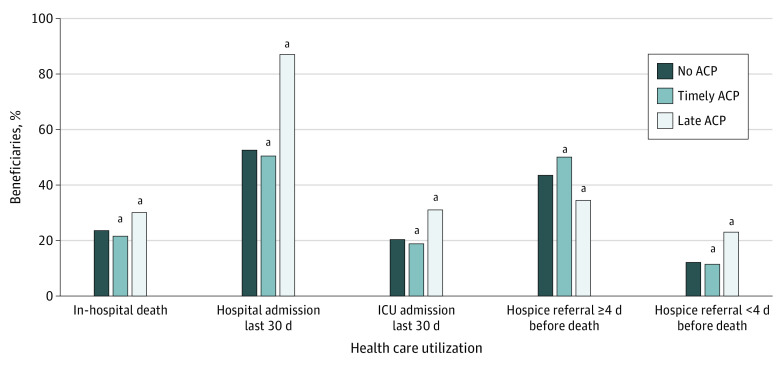
Of the 955 777 Medicare beneficiaries who met criteria for serious illness in 2016 and died in 2017 or 2018, 522 737 (54.7%) were women, 764 666 (80.0%) were 75 years or older, and 822 684 (86.1%) were non-Hispanic White individuals. Among the study population, 81 131 (8.5%) had a timely ACP visit, and an additional 22 804 (2.4%) had a late ACP visit. After multivariable adjustment, compared with patients without any billed ACP visit, patients with a timely ACP visit experienced significantly less intensive EOL care on 4 of 5 measures, including in-hospital death (adjusted odds ratio [aOR], 0.85; 95% CI, 0.84-0.87), hospital admission (aOR, 0.84; 95% CI, 0.83-0.85), intensive care unit admission (aOR, 0.87; 95% CI, 0.85-0.88), and emergency department visit (OR, 0.83; 95% CI, 0.82-0.84). Only small or insignificant differences in late hospice use or mean total EOL expenditures were noted. Compared with patients without ACP, patients with late ACP experienced more intensive EOL care, including in-hospital death (aOR, 1.22; 95% CI, 1.19-1.26), hospital admission (aOR, 5.28; 95% CI, 5.07-5.50), intensive care unit admission (aOR, 1.57; 95% CI, 1.53-1.62), and emergency department visit (aOR, 3.87; 95% CI, 3.72-4.02).
In this cohort study of US Medicare beneficiaries, billed ACP services during the EOL course of patients with serious illness were relatively uncommon, but if they occurred before the last month of life, they were associated with less intensive use of EOL services. Further research on the variables affecting hospice use and expenditures in the EOL period and the differential effect of late ACP is recommended to understand the relative role of ACP in achieving goal-concordant care.
预先医疗指示(ACP)旨在使偏好与生命末期(EOL)护理更加一致,并假定会减少对医疗保健服务的密集使用。 医疗保险和医疗补助服务中心于 2016 年开始为临床医生与患者进行 ACP 讨论提供报销。
确定计费的 ACP 访问是否与 EOL 期间医疗保健服务的密集使用相关。
设计、设置和参与者: 这项对患有重病的患者进行的前瞻性患者水平队列分析包括符合 2016 年 1 月 1 日至 12 月 31 日严重疾病标准并于 2017 年 1 月 1 日至 2018 年 12 月 31 日死亡的 Medicare 收费服务受益人。分析于 2020 年 11 月 1 日至 2021 年 3 月 31 日完成。
使用了五项 EOL 医疗保健服务措施(死亡前 30 天内的住院入院、急诊就诊和/或重症监护病房入住;院内死亡;以及首次临终关怀账单的时间)和一项 EOL 支出措施。分析调整了年龄、种族和民族、性别、Charlson 合并症指数、医疗保险-医疗补助双重资格以及医院转诊区域(高、中、低)的支出。主要暴露是接受计费的 ACP 服务,分为无、及时(死亡前 1 个月以上)或晚期(首次 ACP 就诊≤死亡前 1 个月)。
在符合 2016 年严重疾病标准并于 2017 年或 2018 年死亡的 955777 名 Medicare 受益人中,522737 名(54.7%)为女性,764666 名(80.0%)为 75 岁或以上,822684 名(86.1%)为非西班牙裔白人。在研究人群中,81131 名(8.5%)有及时的 ACP 就诊,另有 22804 名(2.4%)有晚期 ACP 就诊。经过多变量调整后,与没有任何计费 ACP 就诊的患者相比,及时接受 ACP 就诊的患者在五项 EOL 护理措施中的四项上的护理强度明显降低,包括院内死亡(调整后的优势比 [aOR],0.85;95%CI,0.84-0.87)、住院入院(aOR,0.84;95%CI,0.83-0.85)、重症监护病房入院(aOR,0.87;95%CI,0.85-0.88)和急诊就诊(OR,0.83;95%CI,0.82-0.84)。仅观察到晚期临终关怀使用或平均总 EOL 支出的差异较小或无显著差异。与没有 ACP 的患者相比,接受晚期 ACP 的患者接受了更密集的 EOL 护理,包括院内死亡(aOR,1.22;95%CI,1.19-1.26)、住院入院(aOR,5.28;95%CI,5.07-5.50)、重症监护病房入院(aOR,1.57;95%CI,1.53-1.62)和急诊就诊(aOR,3.87;95%CI,3.72-4.02)。
在这项对美国 Medicare 受益人的队列研究中,患者生命末期接受计费的 ACP 服务相对较少,但如果在生命最后一个月之前进行,则与 EOL 服务的使用强度降低相关。建议进一步研究影响 EOL 期间临终关怀使用和支出的变量以及晚期 ACP 的差异效果,以了解 ACP 在实现目标一致护理方面的相对作用。