Department of Neurology, Health Services Research Program, University of Michigan Medical School, Ann Arbor, Michigan, USA.
Department of Neurology, Ann Arbor Veterans Affairs, Ann Arbor, Michigan, USA.
J Am Geriatr Soc. 2020 Nov;68(11):2620-2628. doi: 10.1111/jgs.16730. Epub 2020 Aug 17.
BACKGROUND/OBJECTIVE: Advance care planning (ACP) is associated with improved patient and caregiver outcomes, but is underutilized. To encourage ACP, the Centers for Medicare & Medicaid Services implemented specific ACP visit reimbursement codes in 2016. To better understand the utilization of these ACP reimbursement codes, we explored regional variation in billed ACP visits.
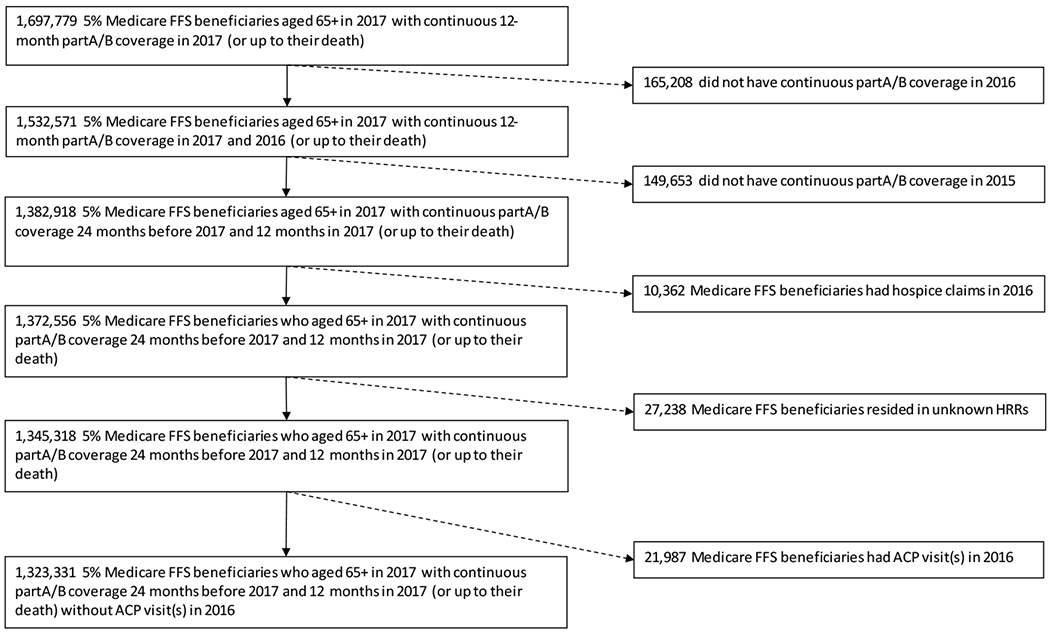
We performed a retrospective cross-sectional analysis using a randomly sampled 5% cohort of Medicare fee-for-service (FFS) beneficiaries' claims files from 2017. Region was defined by hospital referral region.
National Medicare FFS.
A total of 1.3 million Medicare beneficiaries aged 65 years and older.
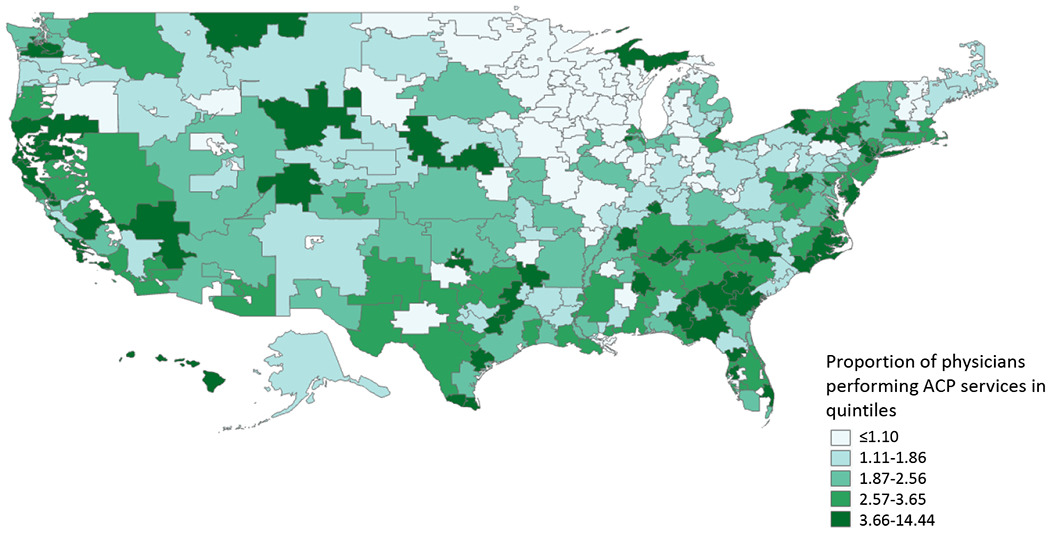
Receipt of billed ACP service, identified through Current Procedural Terminology code 99497 or 99498. Proportion of beneficiaries who received billed ACP service(s) by region was calculated. We fit a multilevel logistic regression model with a random regional intercept to determine the variation in billed ACP visits attributable to the region after accounting for patient (demographics, comorbidities, and medical care utilization) and regional factors (hospital size, emergency department visits, hospice utilization, and costs).
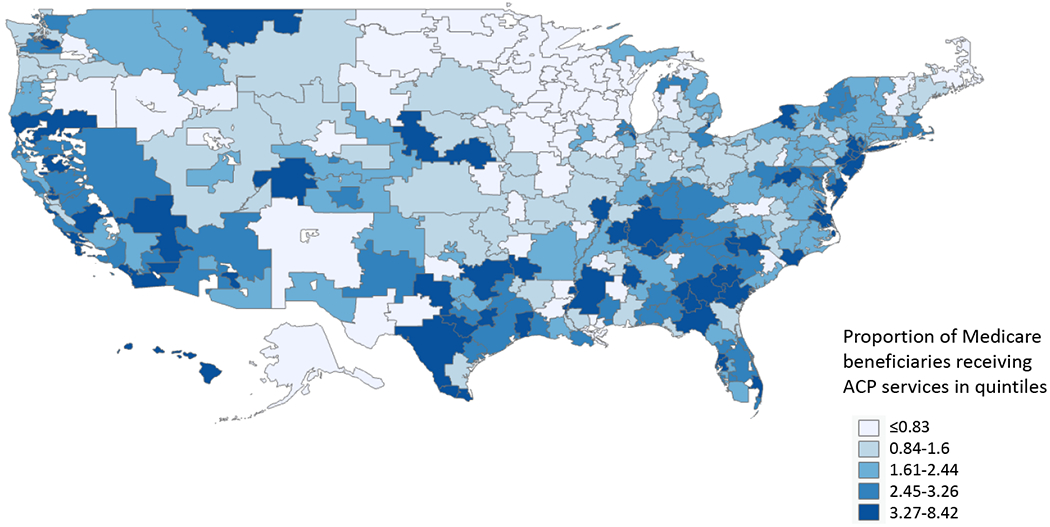
The study population included about 1.3 million beneficiaries, of which 32,137 (2.4%) had at least one billed ACP visit in 2017. There was substantial regional variation in the percentage of beneficiaries with billed ACP visits: lowest quintile region, less than 0.83%; subsequent regions, less than 1.6%, less than 2.4%, less than 3.3% to less than 8.4% in the highest quintile regions. A total of 15.4% of the variance in whether an older adult had a billed ACP visit was explained by the region. Although numerous regional factors were associated with billed ACP visits, none were strong predictors.
In 2017, we found wide regional variation in the use of billed ACP visits, although use overall was low in all regions. Increasing the understanding of the drivers and the effects of billed ACP visits could inform strategies for increasing ACP.
背景/目的:预先医疗指示(ACP)与改善患者和护理人员的预后相关,但利用率较低。为了鼓励 ACP,医疗保险和医疗补助服务中心于 2016 年实施了特定的 ACP 访问报销代码。为了更好地了解这些 ACP 报销代码的使用情况,我们探讨了计费 ACP 访问的区域差异。
我们使用 2017 年医疗保险按服务收费(FFS)受益人的索赔文件的随机抽样 5%队列进行回顾性横断面分析。区域由医院转诊区域定义。
全国医疗保险 FFS。
共有 130 万 65 岁及以上的 Medicare 受益人。
通过当前程序术语代码 99497 或 99498 识别计费 ACP 服务的收据。按区域计算接受计费 ACP 服务的受益人的比例。我们拟合了一个多水平逻辑回归模型,其中包含一个随机区域截距,以确定在考虑患者(人口统计学、合并症和医疗保健利用情况)和区域因素(医院规模、急诊就诊、临终关怀利用情况和成本)后,计费 ACP 就诊的差异归因于区域。
研究人群包括约 130 万受益人,其中 2017 年有 32137 人(2.4%)至少有一次计费 ACP 就诊。接受计费 ACP 就诊的受益人的百分比存在很大的区域差异:最低五分位区域,不到 0.83%;随后的区域,不到 1.6%,不到 2.4%,不到 3.3%到不到 8.4%,最高五分位区域。在老年人是否进行计费 ACP 就诊方面,区域解释了 15.4%的方差。尽管许多区域因素与计费 ACP 就诊相关,但没有一个是强有力的预测因素。
2017 年,我们发现计费 ACP 就诊的使用存在广泛的区域差异,尽管所有区域的使用总体上都较低。增加对计费 ACP 就诊的驱动因素和影响的理解,可以为增加 ACP 的策略提供信息。