Blatter René, Amacher Simon A, Bohren Chantal, Becker Christoph, Beck Katharina, Gross Sebastian, Tisljar Kai, Sutter Raoul, Marsch Stephan, Hunziker Sabina
Medical Communication and Psychosomatic Medicine, University Hospital Basel, Klingelbergstrasse 23, 4031, Basel, Switzerland.
Intensive Care Unit, University Hospital Basel, Basel, Switzerland.
Ann Intensive Care. 2022 Aug 17;12(1):77. doi: 10.1186/s13613-022-01048-y.
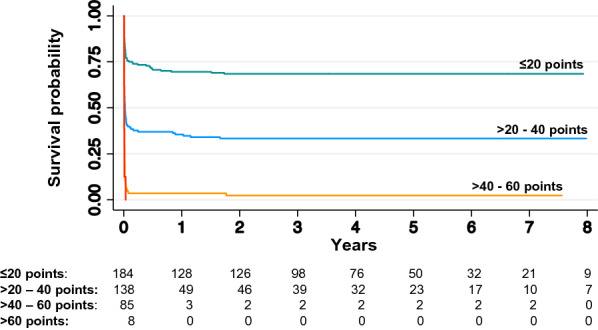
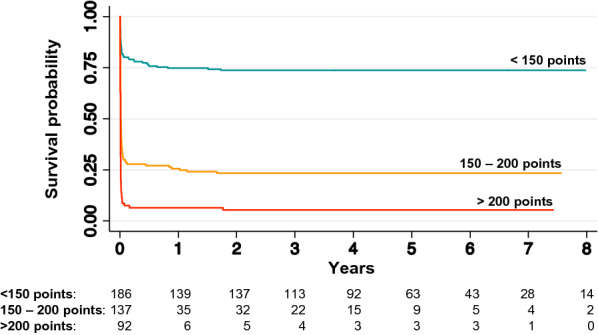
Several scoring systems have been used to predict short-term outcome in patients with out-of-hospital cardiac arrest (OHCA), including the disease-specific OHCA and CAHP (Cardiac Arrest Hospital Prognosis) scores, as well as the general severity-of-illness scores Acute Physiology and Chronic Health Evaluation II (APACHE II) and Simplified Acute Physiology Score II (SAPS II). This study aimed to assess the prognostic performance of these four scores to predict long-term outcomes (≥ 2 years) in adult cardiac arrest patients.
This is a prospective single-centre cohort study including consecutive cardiac arrest patients admitted to intensive care in a Swiss tertiary academic medical centre. The primary endpoint was 2-year mortality. Secondary endpoints were neurological outcome at 2 years post-arrest assessed by Cerebral Performance Category with CPC 1-2 defined as good and CPC 3-5 as poor neurological outcome, and 6-year mortality.
In 415 patients admitted to intensive care, the 2-year mortality was 58.1%, with 96.7% of survivors showing good neurological outcome. The 6-year mortality was 82.5%. All four scores showed good discriminatory performance for 2-year mortality, with areas under the receiver operating characteristics curve (AUROC) of 0.82, 0.87, 0.83 and 0.81 for the OHCA, CAHP, APACHE II and SAPS II scores. The results were similar for poor neurological outcome at 2 years and 6-year mortality.
This study suggests that two established cardiac arrest-specific scores and two severity-of-illness scores provide good prognostic value to predict long-term outcome after cardiac arrest and thus may help in early goals-of-care discussions.
已有多种评分系统用于预测院外心脏骤停(OHCA)患者的短期预后,包括疾病特异性的OHCA评分和CAHP(心脏骤停医院预后)评分,以及一般疾病严重程度评分急性生理与慢性健康状况评估II(APACHE II)和简化急性生理评分II(SAPS II)。本研究旨在评估这四种评分对预测成年心脏骤停患者长期预后(≥2年)的性能。
这是一项前瞻性单中心队列研究,纳入了瑞士一家三级学术医疗中心重症监护病房收治的连续心脏骤停患者。主要终点是2年死亡率。次要终点是心脏骤停后2年的神经功能结局,采用脑功能分类(CPC)评估,CPC 1 - 2定义为良好神经功能结局,CPC 3 - 5为不良神经功能结局,以及6年死亡率。
在415例入住重症监护病房的患者中,2年死亡率为58.1%,96.7%的幸存者神经功能结局良好。6年死亡率为82.5%。所有四种评分对2年死亡率均显示出良好的区分性能,OHCA、CAHP、APACHE II和SAPS II评分的受试者工作特征曲线下面积(AUROC)分别为0.82、0.87、0.83和0.81。对于2年不良神经功能结局和6年死亡率,结果相似。
本研究表明,两种既定的心脏骤停特异性评分和两种疾病严重程度评分对预测心脏骤停后的长期预后具有良好的预后价值,因此可能有助于早期的治疗目标讨论。