Department of Oncology, Faculty of Medicine & Health, Örebro University, 70182, Örebro, SE, Sweden.
Department of Neurosurgery, Faculty of Medicine & Health, Örebro University, 70182, Örebro, SE, Sweden.
Acta Neurochir (Wien). 2022 Nov;164(11):2987-2997. doi: 10.1007/s00701-022-05336-1. Epub 2022 Aug 18.
Meningioma is the most common primary CNS tumour. Most meningiomas are benign, and most patients are 65 years or older. Surgery is usually the primary treatment option. Most prior studies on early surgical outcomes in older patients with meningioma are small, and there is a lack of larger population-based studies to guide clinical decision-making. We aimed to explore the risks for perioperative mortality and morbidity in older patients with meningioma and to investigate changes in surgical incidence over time.
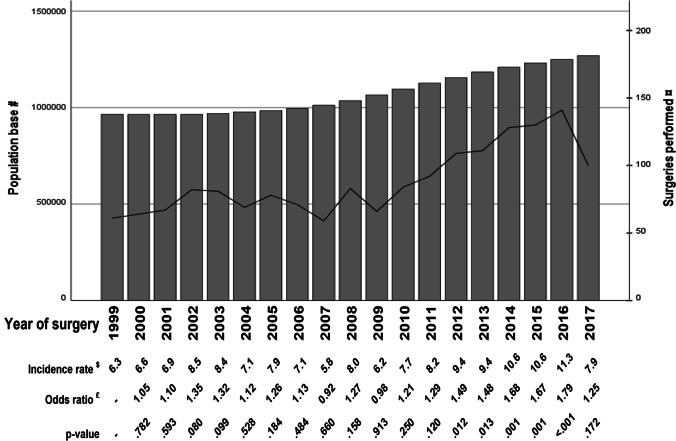
In this retrospective population-based study on patients in Sweden, 65 years or older with surgery 1999-2017 for meningioma, we used data from the Swedish Brain Tumour Registry. We analysed factors contributing to perioperative mortality and morbidity and used official demographic data to calculate yearly incidence of surgical procedures for meningioma.
The final study cohort included 1676 patients with a 3.1% perioperative mortality and a 37.6% perioperative morbidity. In multivariate analysis, higher age showed a statistically significant association with higher perioperative mortality, whereas larger tumour size and having preoperative symptoms were associated with higher perioperative morbidity. A numerical increased rate of surgical interventions after 2012 was observed, without evidence of worsening short-term surgical outcomes.
Higher mortality with increased age and higher morbidity risk in larger and/or symptomatic tumours imply a possible benefit from considering surgery in selected older patients with a growing meningioma before the development of tumour-related symptoms. This study further underlines the need for a standardized method of reporting and classifying complications from neurosurgery.
脑膜瘤是最常见的原发性中枢神经系统肿瘤。大多数脑膜瘤为良性,且大多数患者年龄在 65 岁或以上。手术通常是主要的治疗选择。先前关于老年脑膜瘤患者早期手术结果的大多数研究规模较小,并且缺乏更大的基于人群的研究来指导临床决策。我们旨在探讨老年脑膜瘤患者围手术期死亡率和发病率的风险,并研究手术发病率随时间的变化。
在这项针对瑞典患者的回顾性基于人群的研究中,我们纳入了 1999 年至 2017 年间 65 岁或以上接受脑膜瘤手术的患者,使用了瑞典脑肿瘤登记处的数据。我们分析了导致围手术期死亡率和发病率的因素,并利用官方人口统计数据计算了脑膜瘤手术的年发病率。
最终的研究队列包括 1676 名患者,围手术期死亡率为 3.1%,围手术期发病率为 37.6%。多变量分析显示,较高的年龄与较高的围手术期死亡率具有统计学显著相关性,而较大的肿瘤大小和术前症状与较高的围手术期发病率相关。我们观察到 2012 年后手术干预的比率呈数值增加,但没有证据表明短期手术结果恶化。
随着年龄的增加死亡率增加,且较大和/或有症状的肿瘤发病率风险增加,这意味着对于有不断增大的脑膜瘤且尚未出现与肿瘤相关症状的老年患者,考虑手术可能是有益的。本研究进一步强调了需要一种标准化的方法来报告和分类神经外科手术的并发症。