Department of Physical Medicine & Rehabilitation, Jeonbuk National University Hospital, 20, Geonji-ro, Deokjin-gu, Jeonju-si, Jeollabuk-do, 54907, Republic of Korea.
Research Institute of Clinical Medicine of Jeonbuk National University - Biomedical Research Institute of Jeonbuk National University Hospital, Jeonju, 54907, Republic of Korea.
BMC Neurol. 2022 Aug 18;22(1):303. doi: 10.1186/s12883-022-02795-y.
Polymicrogyria refers to the disruption of normal cerebral cortical development late in neuronal migration or in early cortical organization. Although patients with polymicrogyria feature relatively favorable motor outcomes, polymicrogyric lesions accompanied by extensive unilateral hemispheric atrophy and ipsilateral brainstem atrophy may induce poorer motor outcomes. This study is the first to employ transcranial magnetic stimulation (TMS) and diffusion tensor imaging (DTI) to characterize changes to motor organization and white matter tracts induced by polymicrogyria.
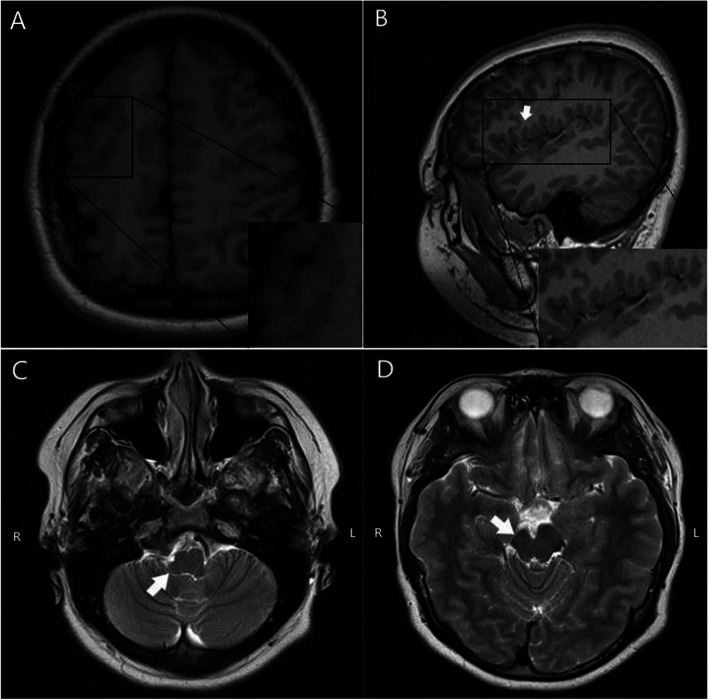
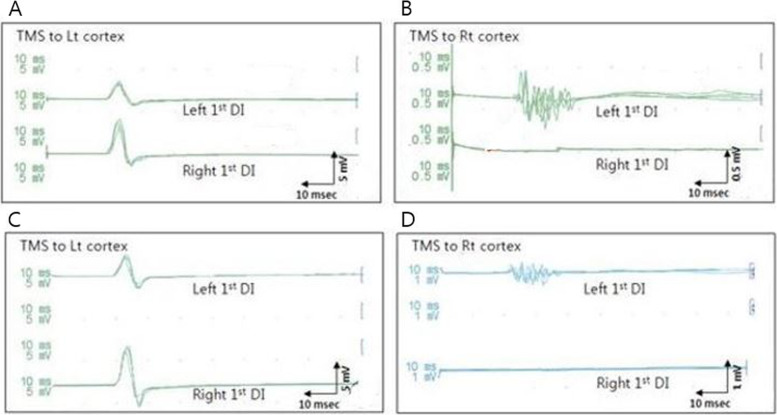
We document a case of a 16-year-old female with left hemiplegic unilateral polymicrogyria associated with ipsilateral brainstem atrophy. Magnetic resonance imaging (MRI) of the brain revealed unilateral polymicrogyria to have affected anterior cortical areas, including the perisylvian region on the right side. The right halves of the brain and brainstem were significantly smaller than the left halves. Although our patient was found to exhibit cortical dysplasia of the right frontoparietal and sylvian fissure areas and a decreased number of fibers in the corticospinal tract (CST) of the affected side on DTI, the connectivity of the CST was preserved up to the motor cortex. We also measured the cross-sectional area of the CST at the level of the pons. In TMS, contralateral motor evoked potentials (MEPs) were evoked from both hands, but the ipsilateral MEPs were evoked only from the left hand. The left hand featured a long duration, polyphasic pattern of contralateral MEPs.
TMS revealed that the concurrent bilateral projections to the paretic hand from the affected and unaffected hemispheres and contralateral MEPs in the paretic hand were polyphasic, indicating delayed electrophysiological maturation or a pathologic condition of the corticospinal motor pathways. In DTI, the cross-sectional area of the CST at the level of the pons on the affected side was smaller than that on the unaffected side. These DTI findings reveal an inadequate CST volume. Despite extensive brain malformation and ipsilateral brainstem atrophy, our patient had less severe motor dysfunction and presented with involuntary mirror movements. Mirror movements in the paretic hand are considered to indicate ipsilateral corticospinal projections from the unaffected hemisphere and may suggest favorable motor outcomes in early brain injury.
多微小脑回畸形是指神经元迁移后期或皮质早期组织过程中皮质正常发育的中断。虽然多微小脑回畸形患者的运动功能预后相对较好,但多微小脑回畸形伴广泛单侧半球萎缩和同侧脑干萎缩可能导致较差的运动功能预后。本研究首次采用经颅磁刺激(TMS)和弥散张量成像(DTI)来描述多微小脑回畸形引起的运动组织和白质束的变化。
我们记录了一例 16 岁女性左偏瘫单侧多微小脑回畸形伴同侧脑干萎缩。脑部磁共振成像(MRI)显示单侧多微小脑回畸形影响了皮质前区,包括右侧大脑外侧裂周围区域。大脑和脑干右侧明显小于左侧。尽管我们的患者在 DTI 上显示右侧额顶和大脑外侧裂区域皮质发育不良,受累侧皮质脊髓束(CST)中的纤维数量减少,但 CST 的连接性一直保持到运动皮质。我们还测量了桥脑水平 CST 的横截面积。在 TMS 中,双手均可引出对侧运动诱发电位(MEPs),但仅左手可引出同侧 MEPs。左手的对侧 MEPs 具有长潜伏期、多相模式。
TMS 显示来自患侧和未患侧半球的双侧投射以及患侧手的对侧 MEPs 呈多相性,这表明皮质脊髓运动通路的电生理成熟延迟或存在病理状态。在 DTI 中,患侧桥脑水平 CST 的横截面积小于健侧。这些 DTI 发现提示 CST 体积不足。尽管大脑畸形广泛且同侧脑干萎缩,但我们的患者运动功能障碍较轻,并出现不自主镜像运动。患侧手的镜像运动被认为是来自未受影响侧半球的同侧皮质脊髓投射的表现,可能提示早期脑损伤的运动功能预后良好。