University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania.
University of Utah School of Medicine, Salt Lake City.
JAMA Health Forum. 2022 Jul 29;3(7):e222263. doi: 10.1001/jamahealthforum.2022.2263. eCollection 2022 Jul.
Prescription opioids can treat acute pain in primary care but have potential for unsafe use and progression to prolonged opioid prescribing.
To compare clinician-facing interventions to prevent unsafe opioid prescribing in opioid-naive primary care patients with acute noncancer pain.
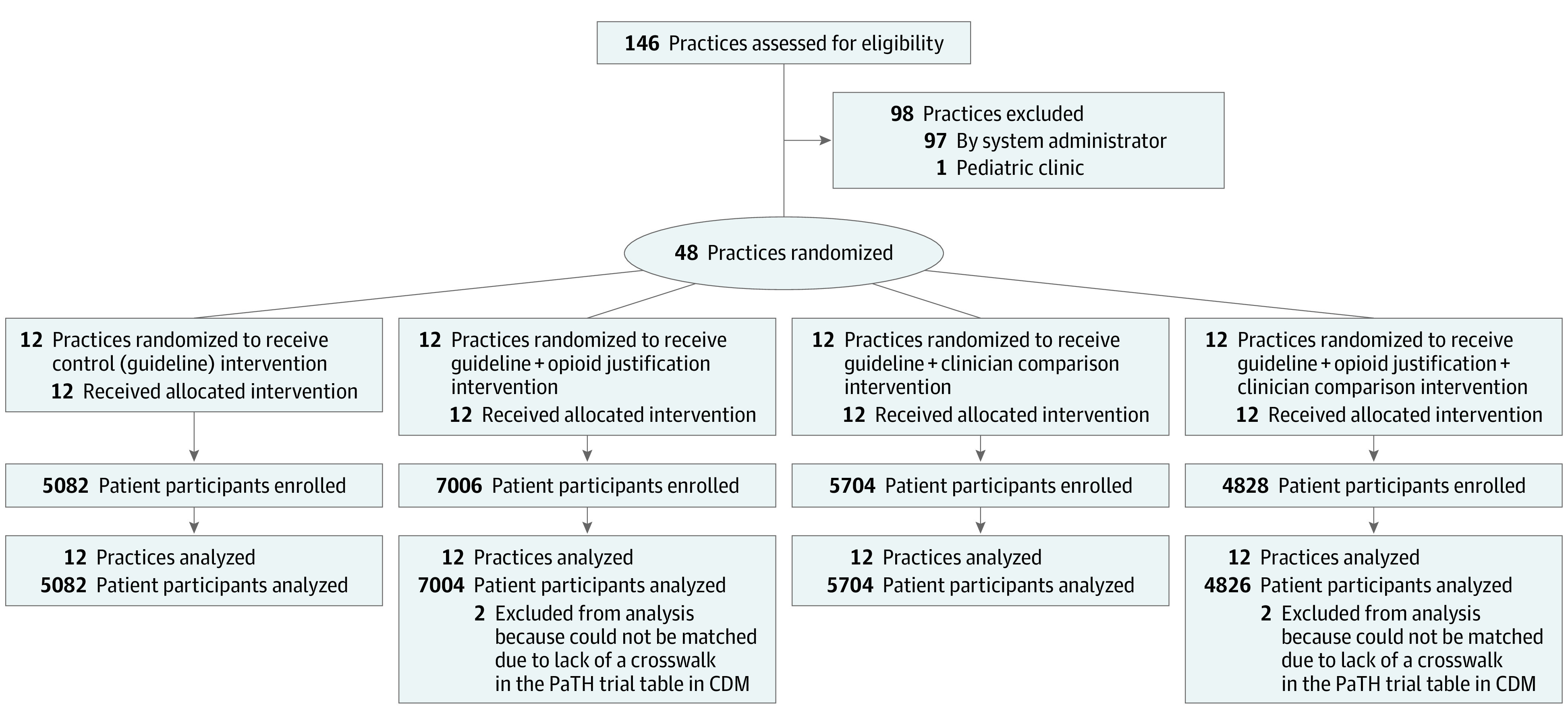
We conducted a multisite, cluster-randomized, 2 × 2 factorial, clinical trial in 3 health care systems that comprised 48 primary care practices and 525 participating clinicians from September 2018 through January 2021. Patient participants were opioid-naive outpatients, 18 years or older, who presented for a qualifying clinic visit with acute noncancer musculoskeletal pain or nonmigraine headache.
Practices randomized to: (1) control; (2) opioid justification; (3) monthly clinician comparison emails; or (4) opioid justification and clinician comparison. All groups received opioid prescribing guidelines via the electronic health record at the time of a new opioid prescription.
Primary outcome measures were receipt of an initial opioid prescription at the qualifying clinic visit. Other outcomes were opioid prescribing for more than 3 months and a concurrent opioid/benzodiazepine prescription over 12-month follow-up.
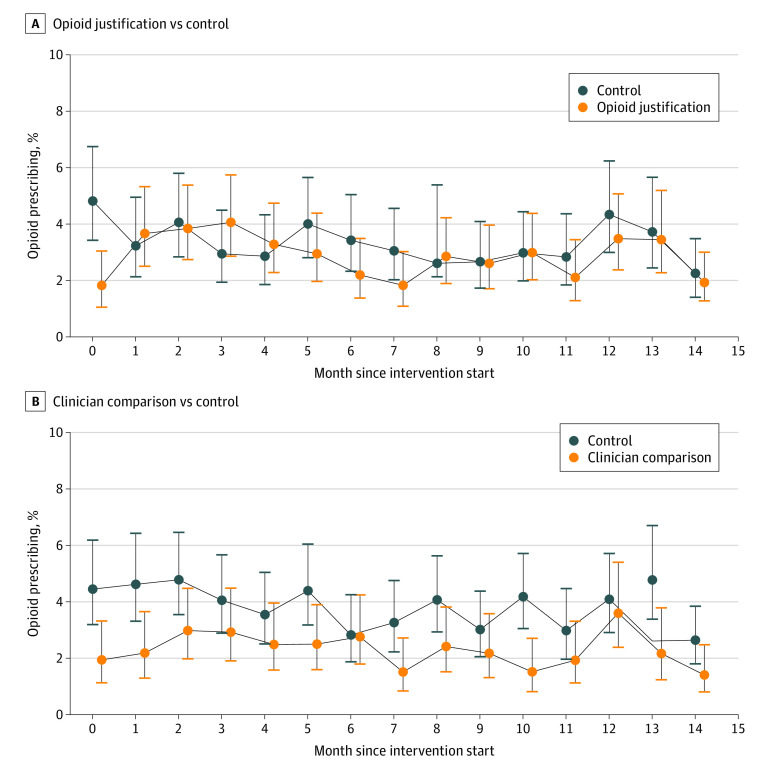
Among 22 616 enrolled patient participants (9740 women [43.1%]; 64 American Indian/Alaska Native [0.3%]; 590 Asian [2.6%], 1120 Black/African American [5.0%], 1777 Hispanic [7.9%], 225 Native Hawaiian/Pacific Islander [1.0%], and 18 981 White [83.9%] individuals), the initial opioid prescribing rates at the qualifying clinic visit were 3.1% in the total sample, 4.2% in control, 3.6% in opioid justification, 2.6% in clinician comparison, and 1.9% in opioid justification and clinician comparison. Compared with control, the adjusted odds ratio (aOR) for a new opioid prescription was 0.74 (95% CI, 0.46-1.18; = .20) for opioid justification and 0.60 (95% CI, 0.38-0.96; = .03) for clinician comparison. Compared with control, clinician comparison was associated with decreased odds of opioid therapy of more than 3 months (aOR, 0.79; 95% CI, 0.69-0.91; = .001) and concurrent opioid/benzodiazepine prescription (aOR, 0.85; 95% CI, 0.72-1.00; = .04), whereas opioid justification did not have a significant effect.
In this cluster randomized clinical trial, comparison emails decreased the proportion of opioid-naive patients with acute noncancer pain who received an opioid prescription, progressed to treatment with long-term opioid therapy, or were exposed to concurrent opioid and benzodiazepine therapy. Health care systems can consider adding clinician-targeted nudges to other initiatives as an efficient, scalable approach to further decrease potentially unsafe opioid prescribing.
ClinicalTrials.gov Identifier: NCT03537573.
处方类阿片药物可用于治疗初级保健中的急性疼痛,但存在不安全使用和延长阿片类药物处方的潜在风险。
比较预防初级保健中无阿片类药物使用史的急性非癌性疼痛患者不安全使用阿片类药物的临床医生干预措施。
设计、设置和参与者:我们在 3 个医疗系统中进行了一项多地点、集群随机、2×2 析因临床试验,该试验包括 48 个初级保健实践和 525 名参与的临床医生,时间为 2018 年 9 月至 2021 年 1 月。患者参与者为无阿片类药物使用史的门诊患者,年龄在 18 岁及以上,因急性非癌性肌肉骨骼疼痛或非偏头痛性头痛就诊。
实践随机分为:(1)对照组;(2)阿片类药物合理性;(3)每月临床医生比较电子邮件;或(4)阿片类药物合理性和临床医生比较。所有组在新的阿片类药物处方时都通过电子健康记录收到阿片类药物处方指南。
主要结局指标是在合格诊所就诊时获得初始阿片类药物处方。其他结局指标为超过 3 个月的阿片类药物处方和 12 个月随访期间同时使用阿片类药物/苯二氮䓬类药物的处方。
在 22616 名入组的患者参与者中(9740 名女性[43.1%];64 名美国印第安人/阿拉斯加原住民[0.3%];590 名亚洲人[2.6%],1120 名黑人/非裔美国人[5.0%],1777 名西班牙裔[7.9%],225 名夏威夷原住民/太平洋岛民[1.0%]和 18981 名白人[83.9%]),合格诊所就诊时的初始阿片类药物处方率在总样本中为 3.1%,在对照组中为 4.2%,在阿片类药物合理性组中为 3.6%,在临床医生比较组中为 2.6%,在阿片类药物合理性和临床医生比较组中为 1.9%。与对照组相比,新阿片类药物处方的调整后优势比(aOR)为 0.74(95%CI,0.46-1.18; = .20),阿片类药物合理性为 0.60(95%CI,0.38-0.96; = .03)。与对照组相比,临床医生比较与减少 3 个月以上阿片类药物治疗的可能性(aOR,0.79;95%CI,0.69-0.91; = .001)和同时使用阿片类药物/苯二氮䓬类药物的可能性(aOR,0.85;95%CI,0.72-1.00; = .04)相关,而阿片类药物合理性没有显著影响。
在这项聚类随机临床试验中,比较电子邮件减少了急性非癌性疼痛且无阿片类药物使用史的患者接受阿片类药物处方、进展为长期阿片类药物治疗或同时使用阿片类药物和苯二氮䓬类药物治疗的比例。医疗保健系统可以考虑将临床医生针对性的提示添加到其他计划中,作为进一步减少潜在不安全阿片类药物处方的有效、可扩展的方法。
ClinicalTrials.gov 标识符:NCT03537573。