Obeidat Adham E, Mahfouz Ratib, Benavente Kevin, Kozai Landon A, Mansour Mahmoud M, Darweesh Mohammad, Pyrsopoulos Nikolaos T
Hepatology, Rutgers University New Jersey Medical School, Newark, USA.
Internal Medicine, Kent Hospital/Brown University, Warwick, USA.
Cureus. 2022 Jul 18;14(7):e26964. doi: 10.7759/cureus.26964. eCollection 2022 Jul.
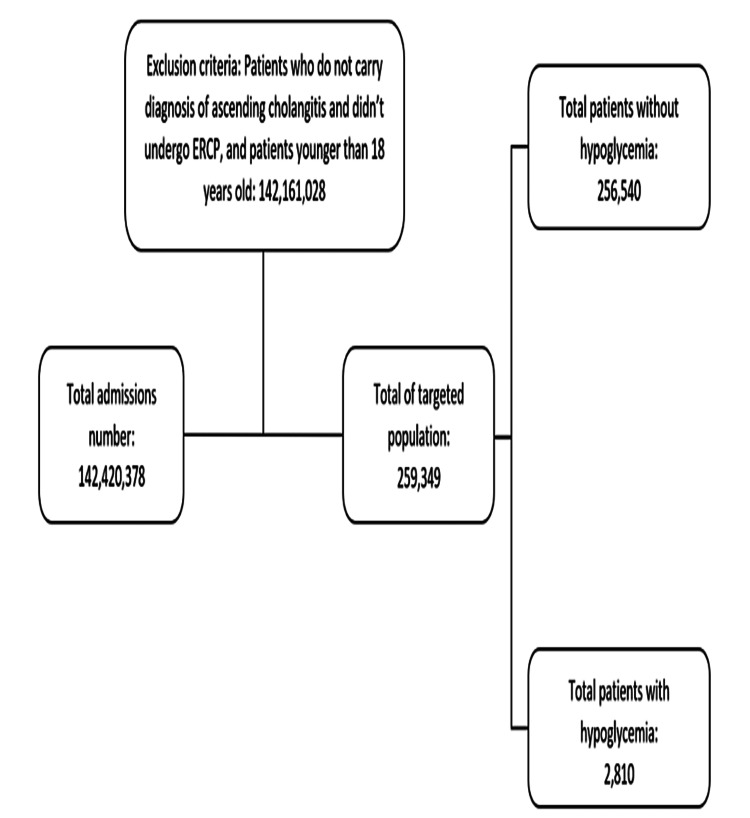
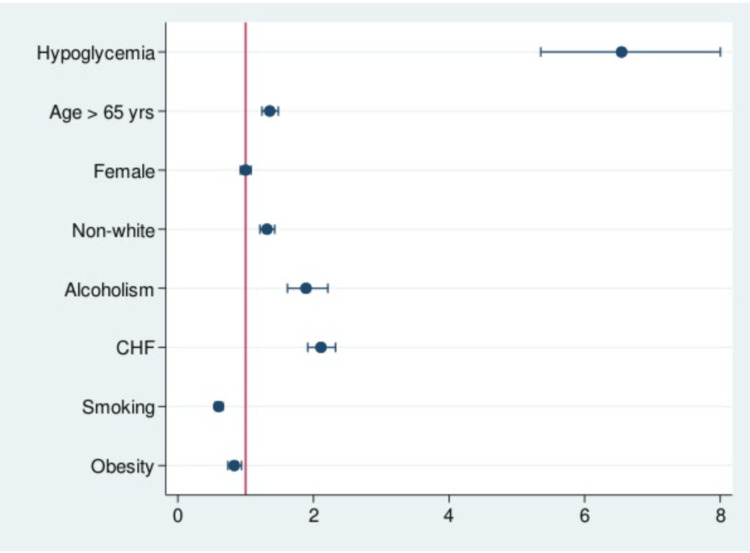
Background Hypoglycemia has been associated with poorer outcomes in hospitalized patients undergoing surgical interventions. In cholangitis, endoscopic retrograde cholangiopancreatography (ERCP) is often a critical adjunct to surgery, capable of diagnosing and treating various biliary and pancreatic pathologies. While technically less invasive than surgery, the effect of hypoglycemia on clinical outcomes of patients with cholangitis undergoing ERCP has not been elucidated. Methodology Data were extracted from the National Inpatient Sample (NIS) database from 2016 to 2019. Using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes, patients diagnosed with cholangitis and underwent ERCP were identified. Baseline demographic data, comorbidities, in-hospital mortality, hospital charges, and hospital length of stay (LOS) were extracted and compared based on the presence or absence of hypoglycemia. Statistical analysis was done using t-test and chi-square analyses. A multivariate analysis for the mortality odds ratio (OR) was calculated to adjust for possible confounders. Results A total of 256,540 patients with cholangitis who underwent ERCP were identified, and 2,810 of them had hypoglycemia during their hospitalization. The mean age of the hypoglycemia group was 64.41 years. Most patients were females (54%) and whites (57%). More patients in the hypoglycemia group had a history of alcoholism and congestive heart failure (CHF). Hypoglycemia was associated with higher odds of in-hospital mortality (OR = 6.71, confidence interval (CI) = 5.49-8.2; p < 0.0001). In addition to hypoglycemia, age >65 years, non-white race, and CHF were independently associated with higher mortality. Moreover, patients with hypoglycemia had higher total hospital charges ($87,147 vs. $133,400; p < 0.0001) and a significant increase in the LOS (9.7 vs. 6.7 days; p < 0.0001). Conclusions Previous studies in the surgical literature have linked hypoglycemia to increased incidence of atrial fibrillation, usage of mechanical ventilation, and application of circulatory support. Hypoglycemia may also affect the metabolism of the heart, leading to myocardial ischemia and malignant arrhythmias. However, it is unclear if hypoglycemia represents a proxy for the severity of patient illness as septic shock and renal insufficiency are common etiologies that may strongly impact mortality. Therefore, careful glycemic control during hospitalization should be practiced as hypoglycemia serves as a poor prognostic indicator that should not be overlooked.
低血糖与接受手术干预的住院患者较差的预后相关。在胆管炎中,内镜逆行胰胆管造影术(ERCP)通常是手术的关键辅助手段,能够诊断和治疗各种胆道和胰腺疾病。虽然在技术上比手术侵入性小,但低血糖对接受ERCP的胆管炎患者临床结局的影响尚未阐明。
从2016年至2019年的国家住院样本(NIS)数据库中提取数据。使用国际疾病分类第十版临床修订本(ICD-10-CM)编码,识别出诊断为胆管炎并接受ERCP的患者。根据是否存在低血糖,提取并比较基线人口统计学数据、合并症、住院死亡率、住院费用和住院时间(LOS)。使用t检验和卡方分析进行统计分析。计算死亡率比值比(OR)的多变量分析以调整可能的混杂因素。
共识别出256,540例接受ERCP的胆管炎患者,其中2,810例在住院期间发生低血糖。低血糖组的平均年龄为64.41岁。大多数患者为女性(54%)和白人(57%)。低血糖组中更多患者有酗酒和充血性心力衰竭(CHF)病史。低血糖与住院死亡率较高相关(OR = 6.71,置信区间(CI)= 5.49 - 8.2;p < 0.0001)。除低血糖外,年龄>65岁、非白人种族和CHF与较高死亡率独立相关。此外,低血糖患者的总住院费用更高(87,147美元对133,400美元;p < 0.0001),住院时间显著增加(9.7天对6.7天;p < 0.0001)。
外科文献中的先前研究已将低血糖与房颤发生率增加、机械通气使用和循环支持应用联系起来。低血糖也可能影响心脏代谢,导致心肌缺血和恶性心律失常。然而,尚不清楚低血糖是否代表患者疾病严重程度的替代指标,因为感染性休克和肾功能不全是可能强烈影响死亡率的常见病因。因此,住院期间应谨慎进行血糖控制,因为低血糖是一个不应被忽视的不良预后指标。