Ibrahim Ramy, Yadav Swarada, Waqar Sumaita, Hermann Jose Ruben, Sarwar Abeer, Shah Sundeep
Research, Premier Medical Associates, The Villages, USA.
Internal Medicine, University of Alabama at Birmingham, The Villages, USA.
Cureus. 2022 Jul 18;14(7):e26994. doi: 10.7759/cureus.26994. eCollection 2022 Jul.
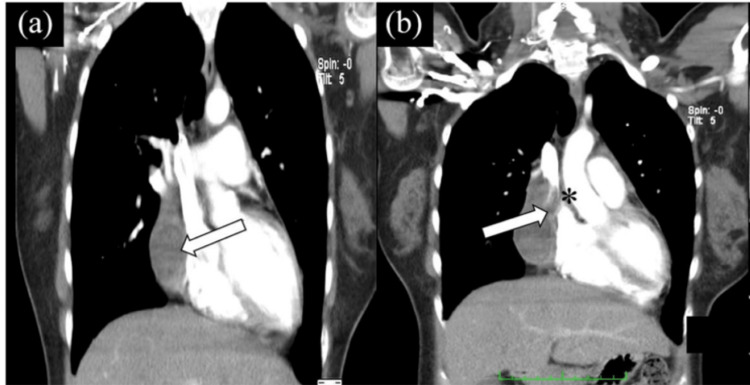
The superior vena cava syndrome (SVCS) has been frequently reported to be secondary to malignancy, specifically, small cell bronchogenic carcinoma and non-Hodgkin's lymphoma. There is some data suggesting causes like postprocedural hematomas. We aim to describe a case of a patient who developed SVCS secondary to a mediastinal hematoma secondary to epicardial pacer leads (postprocedural). Our case is about a 75-year-old male with a past medical history of coronary artery disease and coronary artery bypass graft (CABG) who presented to the Emergency Department (ED) with moderate-to-severe right axillary pain radiating to the ipsilateral side of the neck, arm, and chest, associated to right temporal headache. A computed tomography angiography (CTA) of the chest was indicated at the time and revealed a hematoma with an active extravasation within the right superior anterior mediastinum, outside the pericardium. The patient was admitted to the Cardiovascular Intensive Care Unit (CVICU) and was started on nicardipine as his blood pressure in the ED was 217/125 and remained elevated despite proper pain management. A repeat CT scan of the chest showed a regressing hematoma that coincided with an improvement of the symptoms. This case highlights the importance of the complications of anterior mediastinal hematoma. The superior vena cava syndrome can develop after cardiologic procedures, after the implantation of devices. Prompt clinical diagnosis, including imaging, and treatment are necessary to manage this condition.
上腔静脉综合征(SVCS)经常被报道继发于恶性肿瘤,特别是小细胞支气管肺癌和非霍奇金淋巴瘤。有一些数据表明其病因如术后血肿。我们旨在描述一例患者,其发生SVCS继发于心外膜起搏器导线置入术后(术后)的纵隔血肿。我们的病例是一名75岁男性,有冠状动脉疾病和冠状动脉旁路移植术(CABG)病史,因中度至重度右腋窝疼痛放射至同侧颈部、手臂和胸部,并伴有右侧颞部头痛而就诊于急诊科(ED)。当时进行了胸部计算机断层血管造影(CTA),显示右上前纵隔心包外有一血肿并有活动性外渗。患者被收入心血管重症监护病房(CVICU),因在急诊科时血压为217/125,尽管进行了适当的疼痛管理但仍持续升高,故开始使用尼卡地平治疗。胸部重复CT扫描显示血肿逐渐消退,症状也随之改善。该病例突出了前纵隔血肿并发症的重要性。上腔静脉综合征可在心脏手术、器械植入后发生。及时的临床诊断,包括影像学检查和治疗对于处理这种情况是必要的。