Shelley Ben, McCall Philip, Glass Adam, Orzechowska Izabella, Klein Andrew
University of Glasgow Academic Unit of Anaesthesia, Pain and Critical Care Medicine, Glasgow, United Kingdom.
Department of Cardiothoracic Anaesthesia and Intensive Care, Golden Jubilee National Hospital, Clydebank, United Kingdom.
JTCVS Open. 2022 Jan 25;9:281-290. doi: 10.1016/j.xjon.2022.01.018. eCollection 2022 Mar.
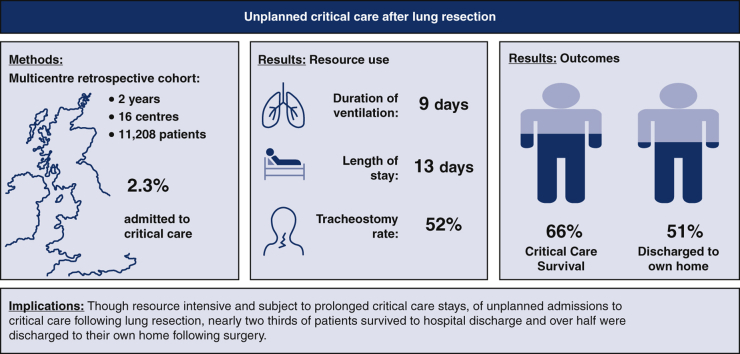
Patients undergoing lung resection are at risk of perioperative complications, many of which necessitate unplanned critical care unit admission in the postoperative period. We sought to characterize this population, providing an up-to-date estimate of the incidence of unplanned critical care admission, and to assess critical care and hospital stay, resource use, mortality, and outcomes.
A multicenter retrospective cohort study of patients undergoing lung resection in participating UK hospitals over 2 years. A comprehensive dataset was recorded for each critical care admission (defined as the need for intubation and mechanical ventilation and/or renal replacement therapy), in addition to a simplified dataset in all patients undergoing lung resection during the study period. Multivariable regression analysis was used to identify factors independently associated with critical care outcome.
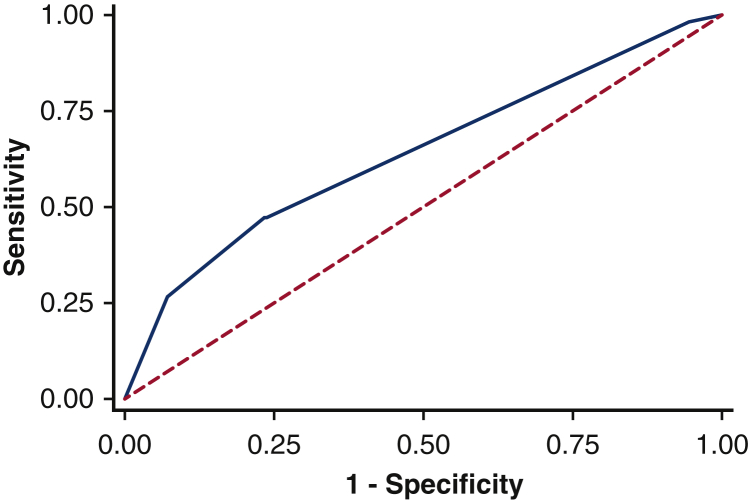
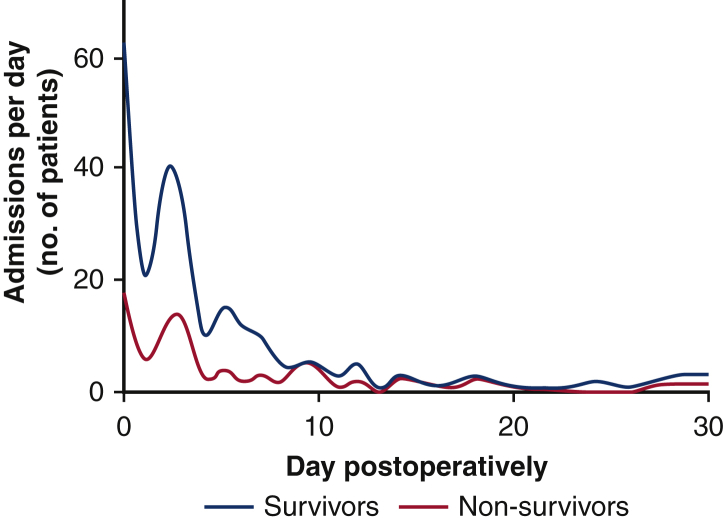
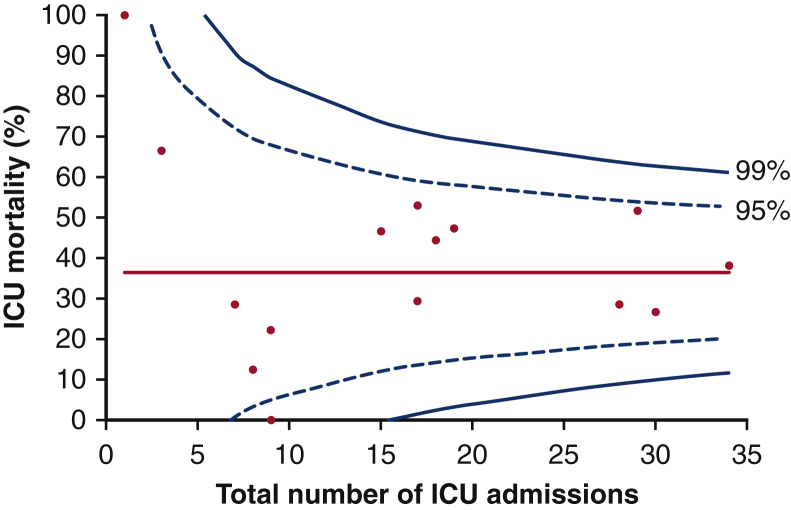
A total of 11,208 patients underwent lung resection in 16 collaborating centers during the study period, and 253 patients (2.3%) required unplanned critical care admission with a median duration of stay of 13 (4-28) days. The predominant indication for admission was respiratory failure (68.1%), with 77.8% of patients admitted during the first 7 days following surgery. Eighty-seven (34.4%) died in critical care. On multivariable regression, only the diagnosis of right ventricular dysfunction and the need for both mechanical ventilation and renal-replacement therapy were independently associated with critical care survival; this model, however, had poor predictive value.
Although resource-intensive and subject to prolonged stay, following unplanned admission to critical care after lung resection outcomes are good for many patients; 65.6% of patients survived to hospital discharge, and 62.7% were discharged to their own home.
接受肺切除术的患者存在围手术期并发症风险,其中许多并发症需要患者在术后非计划入住重症监护病房。我们旨在描述这一人群的特征,提供非计划入住重症监护病房发生率的最新估计,并评估重症监护情况、住院时间、资源利用、死亡率和结局。
一项对英国参与研究的医院中接受肺切除术的患者进行的多中心回顾性队列研究,为期2年。除了记录研究期间所有接受肺切除术患者的简化数据集外,还为每次重症监护病房入住(定义为需要插管和机械通气和/或肾脏替代治疗)记录了一个综合数据集。采用多变量回归分析来确定与重症监护结局独立相关的因素。
在研究期间,16个合作中心共有11208例患者接受了肺切除术,253例患者(2.3%)需要非计划入住重症监护病房,中位住院时间为13(4 - 28)天。入住的主要原因是呼吸衰竭(68.1%),77.8%的患者在术后前7天内入住。87例(34.4%)患者在重症监护病房死亡。在多变量回归分析中,只有右心室功能障碍的诊断以及同时需要机械通气和肾脏替代治疗与重症监护病房存活独立相关;然而,该模型的预测价值较差。
尽管肺切除术后非计划入住重症监护病房资源消耗大且住院时间长,但对许多患者来说结局良好;65.6%的患者存活至出院,62.7%的患者出院后回家。