Lo Theresa, Schiller Robin, Raghunathan Karthik, Krishnamoorthy Vijay, Jawitz Oliver K, Pyati Srinivas, Van De Ven Thomas, Bartz Raquel R, Thompson Annemarie, Ohnuma Tetsu
Critical Care and Perioperative Population Health Research (CAPER) Unit, Department of Anesthesiology, Duke University Medical Center, Durham, NC.
Division of Critical Care Medicine, Department of Anesthesiology, Duke University Medical Center, Durham, NC.
JTCVS Open. 2021 Mar 26;6:224-236. doi: 10.1016/j.xjon.2021.03.015. eCollection 2021 Jun.
To evaluate trends in the use of epidural analgesia and nonopioid and opioid analgesics for patients undergoing lobectomy from 2009 to 2018.
We queried the Premier database for adult patients undergoing open, video-assisted, and robotic-assisted lobectomy from 2009 to 2018. The outcome of interest was changes in the receipt of epidural analgesia and nonopioid and opioid analgesics as measured by charges on the day of surgery. We also evaluated postoperative daily opioid use. We used multivariable logistic and linear regression models to examine the association between the utilization of each analgesic modality and year.
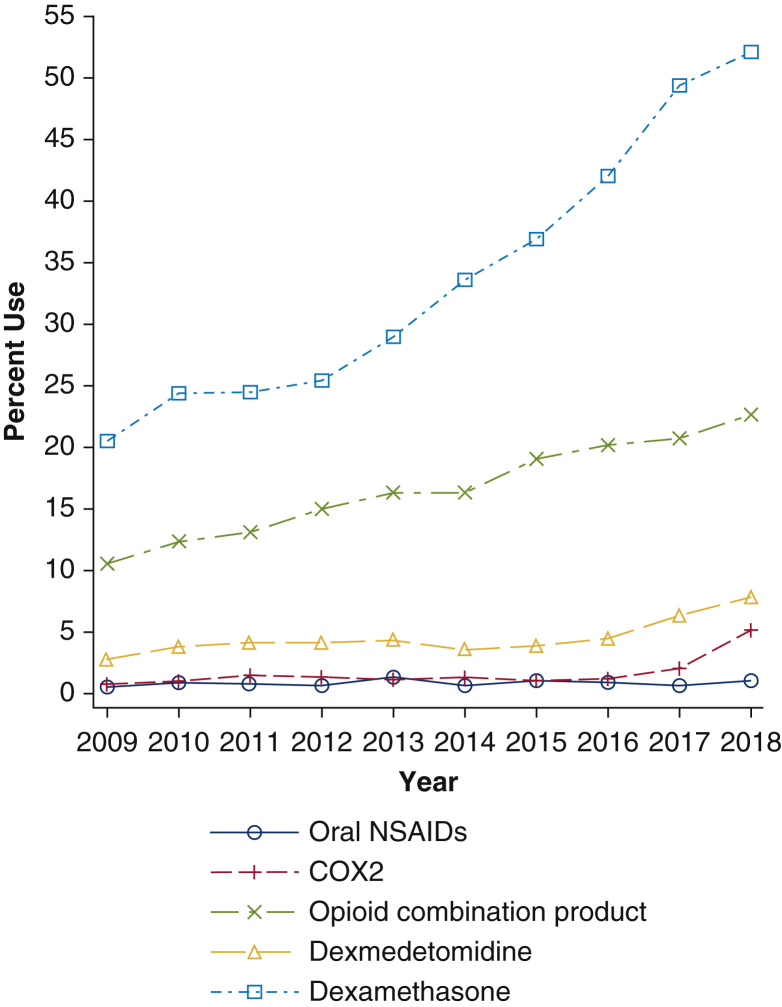
We identified 86,308 patients undergoing lobectomy from 2009 to 2018 within the Premier database: 35,818 (41.5%) patients had open lobectomy, 35,951 (41.7%) patients had video-assisted lobectomy, and 14,539 (16.8%) patients had robotic-assisted lobectomy. For all 3 surgical cohorts, epidural analgesia use decreased, and nonopioid analgesics use increased over time, except for intravenous nonsteroidal anti-inflammatory drugs. Use of patient-controlled analgesia decreased, while opioid consumption on the day of surgery increased and postoperative opioid consumption did not decrease over time.
In this large sample of patients undergoing lobectomy, utilization of epidural analgesia declined and use of nonopioid analgesics increased. Despite these changes, opioid consumption on day of surgery increased, and there was no significant reduction in postoperative opioid consumption. Further research is warranted to examine the association of these changes with patient outcomes.
评估2009年至2018年接受肺叶切除术患者使用硬膜外镇痛以及非阿片类和阿片类镇痛药的趋势。
我们查询了Premier数据库中2009年至2018年接受开放、电视辅助和机器人辅助肺叶切除术的成年患者。感兴趣的结果是通过手术当天的费用衡量的硬膜外镇痛以及非阿片类和阿片类镇痛药使用情况的变化。我们还评估了术后每日阿片类药物的使用情况。我们使用多变量逻辑回归和线性回归模型来研究每种镇痛方式的使用与年份之间的关联。
我们在Premier数据库中确定了2009年至2018年期间86308例接受肺叶切除术的患者:35818例(41.5%)患者接受了开放肺叶切除术,35951例(41.7%)患者接受了电视辅助肺叶切除术,14539例(16.8%)患者接受了机器人辅助肺叶切除术。对于所有3个手术队列,随着时间的推移,硬膜外镇痛的使用减少,非阿片类镇痛药的使用增加,但静脉注射非甾体抗炎药除外。患者自控镇痛的使用减少,而手术当天阿片类药物的消耗量增加,术后阿片类药物的消耗量并未随时间减少。
在这个接受肺叶切除术的大量患者样本中,硬膜外镇痛的使用减少,非阿片类镇痛药的使用增加。尽管有这些变化,手术当天阿片类药物的消耗量增加,术后阿片类药物的消耗量没有显著减少。有必要进行进一步研究以检查这些变化与患者预后的关联。