Bianco Valentino, Kilic Arman, Aranda-Michel Edgar, Serna-Gallegos Derek, Dunn-Lewis Courtenay, Chen Shangzhen, Thoma Floyd, Navid Forozan, Sultan Ibrahim
Division of Cardiac Surgery, Department of Cardiothoracic Surgery, University of Pittsburgh, Pittsburgh, Pa.
Heart and Vascular Institute, University of Pittsburgh Medical Center, Pittsburgh, Pa.
JTCVS Open. 2021 Jun 16;7:157-164. doi: 10.1016/j.xjon.2021.06.005. eCollection 2021 Sep.
Permanent pacemaker placement (PPM) is associated with morbidity following cardiac surgery. This study identified associations between PPM placement and 5-year outcomes for patients that require PPM following valvular surgery.
All patients who underwent valvular surgery at our medical center from 2011 to 2018 were considered for analysis. Multivariable analysis identified associations between PPM placement, mortality, and readmissions. Primary outcomes were operative complications and mortality. Secondary outcomes included 5-year survival and readmission.
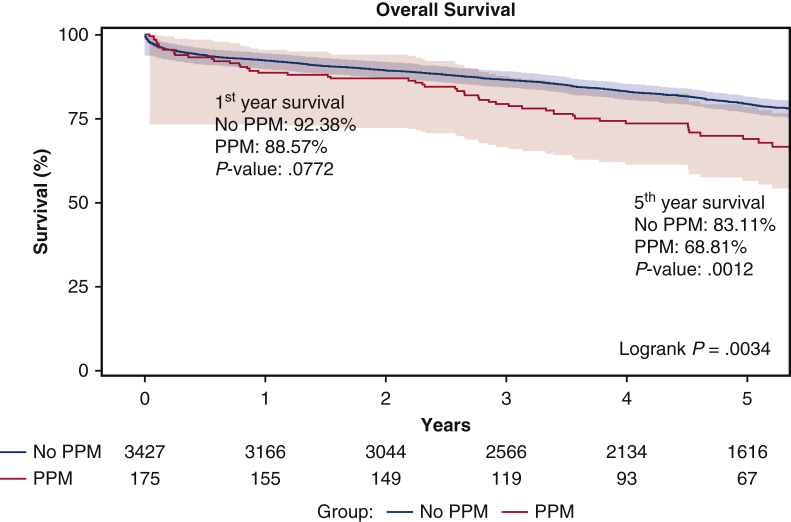
A total of 175 (4.86%) of 3602 valvular surgery patients required postoperative PPM. The PPM cohort had significantly worse baseline comorbidities, including greater Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM) scores (3.8 vs 2.4 < .0001). The PPM cohort had greater rates of blood product transfusion, prolonged ventilation, and new-onset atrial fibrillation. PPM placement was significantly associated with third-degree heart block (5.26; 95% confidence interval [95% CI], 1.00-27.53; = .0496), ventricular fibrillation/tachycardia (3.90; 95% CI, 1.59-9.59; = .01), and atrial fibrillation/flutter (1.53; 95% CI, 1.05-2.24; = .03). On Kaplan-Meier estimates, 5-year survival (68.8% vs 83.1%; = 01) was significantly reduced in the PPM cohort. Five-year all-cause readmission (60.4% vs 50.04%; = .01) and heart failure readmission (35.5% vs 20.1%; < .000) occurred more frequently in the PPM cohort. On multivariable Cox regression analysis, PPM placement (hazard ratio, 1.12; 95% CI, 0.84-1.50; = .444) was not an independent predictor of mortality. On competing risk analysis, PPM (hazard ratio, 1.33; 95% CI, 0.99-1.80; = .062) was not a predictor of hospital readmission.
Valvular surgery patients who required postoperative PPM had elevated baseline operative risk. However, PPM implantation was not associated with mortality or readmission.
永久性起搏器植入(PPM)与心脏手术后的发病率相关。本研究确定了瓣膜手术后需要PPM的患者中PPM植入与5年预后之间的关联。
对2011年至2018年在我们医疗中心接受瓣膜手术的所有患者进行分析。多变量分析确定了PPM植入、死亡率和再入院之间的关联。主要结局为手术并发症和死亡率。次要结局包括5年生存率和再入院率。
3602例瓣膜手术患者中有175例(4.86%)术后需要PPM。PPM队列的基线合并症明显更严重,包括更高的胸外科医师协会预测死亡率(STS-PROM)评分(3.8对2.4,<0.0001)。PPM队列的血液制品输注率、通气时间延长和新发房颤发生率更高。PPM植入与三度房室传导阻滞(5.26;95%置信区间[95%CI],1.00-27.53;P=0.0496)、室颤/室速(3.90;95%CI,1.59-9.59;P=0.01)和房颤/房扑(1.53;95%CI,1.05-2.24;P=0.03)显著相关。根据Kaplan-Meier估计,PPM队列的5年生存率(68.8%对83.1%;P=0.01)显著降低。PPM队列的5年全因再入院率(60.4%对50.04%;P=0.01)和心力衰竭再入院率(35.5%对20.1%;P<0.000)更高。多变量Cox回归分析显示,PPM植入(风险比,1.12;95%CI,0.84-1.50;P=0.444)不是死亡率的独立预测因素。竞争风险分析显示,PPM(风险比,1.33;95%CI,0.99-1.80;P=0.062)不是医院再入院的预测因素。
瓣膜手术后需要PPM的患者基线手术风险升高。然而,PPM植入与死亡率或再入院无关。